Potrebbero piacerti anche
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Anatomy of The Chest WallDocumento10 pagineAnatomy of The Chest WallJ C Campus PonnyNessuna valutazione finora
- Geriatric Case StudyDocumento15 pagineGeriatric Case StudyJobelle AcenaNessuna valutazione finora
- Thoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دDocumento18 pagineThoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دMuhammad UsmanNessuna valutazione finora
- The Pathway: The Human Respiratory SystemDocumento25 pagineThe Pathway: The Human Respiratory SystemKenneth Decker PrietoNessuna valutazione finora
- 1) Anatomy & Physiology - 202243.15374-CCRN-1505-01 - MANAGEMENT OF CCHC - RESPIRATORYDocumento12 pagine1) Anatomy & Physiology - 202243.15374-CCRN-1505-01 - MANAGEMENT OF CCHC - RESPIRATORYafshin nikraveshNessuna valutazione finora
- Assessment of Lungs and ThoraxDocumento58 pagineAssessment of Lungs and ThoraxShahmeerNessuna valutazione finora
- Pneumothorax (Collapsed Lung)Documento34 paginePneumothorax (Collapsed Lung)james garcia100% (3)
- Hemothorax HandoutsDocumento2 pagineHemothorax HandoutsJunathan L. DelgadoNessuna valutazione finora
- Pleura Space Anatomy: Review ArticleDocumento6 paginePleura Space Anatomy: Review ArticleRohitNessuna valutazione finora
- Azygous VeinDocumento12 pagineAzygous VeinLorenz SmallNessuna valutazione finora
- Anatomy of The Heart: Epicardium Myocardium EndocardiumDocumento8 pagineAnatomy of The Heart: Epicardium Myocardium EndocardiumTrishna ShahNessuna valutazione finora
- Case Study - Septic ShockDocumento16 pagineCase Study - Septic ShockIrene Mae Villanueva Ariola100% (2)
- Overview of Visceral Thorax - PleuraDocumento33 pagineOverview of Visceral Thorax - PleuraHrishikesh BirjeNessuna valutazione finora
- THORAX Part 2Documento59 pagineTHORAX Part 2idrimuha333Nessuna valutazione finora
- Pleural EffusionDocumento53 paginePleural EffusionZhyraine Iraj D. CaluzaNessuna valutazione finora
- Unit 6 Part 2 Thoracic CavityDocumento56 pagineUnit 6 Part 2 Thoracic CavitySiraj ShiferawNessuna valutazione finora
- Acute Respiratory Distres SyndromeDocumento17 pagineAcute Respiratory Distres SyndromeLalrinchhani PautuNessuna valutazione finora
- General Anatomy 4 Thoracic Cavity: Dr. Wesam BaderDocumento46 pagineGeneral Anatomy 4 Thoracic Cavity: Dr. Wesam BaderAhmadNessuna valutazione finora
- Review of LiteratureDocumento33 pagineReview of LiteratureMahmmoud EltaweelNessuna valutazione finora
- Ribs Vertebral Column Sternum Abdominal Cavity Diaphragm Lungs Heart Blood Arteries VeinsDocumento11 pagineRibs Vertebral Column Sternum Abdominal Cavity Diaphragm Lungs Heart Blood Arteries VeinsHamda HassanNessuna valutazione finora
- Respiratory AssessmentDocumento25 pagineRespiratory AssessmentLIBIN PALLUPPETTAYIL JOSE100% (2)
- Ch.19 Thorax and LungsDocumento14 pagineCh.19 Thorax and LungsJose R. MendozaNessuna valutazione finora
- Respiratory: Welcome!Documento119 pagineRespiratory: Welcome!Majo ParagasNessuna valutazione finora
- BY Ifenna Nnachi Salvator REG NO: 2019070000636Documento35 pagineBY Ifenna Nnachi Salvator REG NO: 2019070000636nnachi ifennaNessuna valutazione finora
- Seminar On: Pulmonary TuberculosisDocumento33 pagineSeminar On: Pulmonary TuberculosisPriyaranjan Jose86% (7)
- Chestx RayinterpretationDocumento81 pagineChestx RayinterpretationTIRUCHANURUNessuna valutazione finora
- BronchiectasisDocumento71 pagineBronchiectasisvijay1234568883Nessuna valutazione finora
- Respiratory SystemDocumento17 pagineRespiratory SystemkimberlynNessuna valutazione finora
- Bronchial Asthma ThesisDocumento33 pagineBronchial Asthma ThesisAbdul Hafiz40% (5)
- Chest X-Ray ReviewDocumento145 pagineChest X-Ray ReviewHamid ShaalanNessuna valutazione finora
- Lessonplan FinDocumento14 pagineLessonplan Finx483xDNessuna valutazione finora
- Bronchial AsthmaDocumento21 pagineBronchial AsthmaMoonNessuna valutazione finora
- Checklist 3Documento9 pagineChecklist 3FranklinSappNessuna valutazione finora
- تجميع اول محاضره RespiratoryDocumento9 pagineتجميع اول محاضره RespiratoryAhmed KadiraNessuna valutazione finora
- Lung AnatomyDocumento19 pagineLung AnatomyScott Yee100% (2)
- Var 29 - 30Documento4 pagineVar 29 - 30Honey BabaNessuna valutazione finora
- Lungs-WPS OfficeDocumento23 pagineLungs-WPS Officezenith parmarNessuna valutazione finora
- Anatomy of Pluera, Lungs and The Tracheobroncial TreeDocumento108 pagineAnatomy of Pluera, Lungs and The Tracheobroncial TreeTahleel AltafNessuna valutazione finora
- Respiratory SystemDocumento56 pagineRespiratory SystemSalma NawazNessuna valutazione finora
- MED 1.4 PE of The Chest, Lungs, Breast, and Axilla PDFDocumento16 pagineMED 1.4 PE of The Chest, Lungs, Breast, and Axilla PDFelleinasNessuna valutazione finora
- Embryology, Gross Anatomy and Histology of Lungs and Pleura: For PC-II Medicine Students By: Zelalem ADocumento58 pagineEmbryology, Gross Anatomy and Histology of Lungs and Pleura: For PC-II Medicine Students By: Zelalem AAmanuel MaruNessuna valutazione finora
- Chest X Rays Made EasyDocumento3 pagineChest X Rays Made EasyHaluk AlibazogluNessuna valutazione finora
- Oxygenation and Airway Management: Quick LookDocumento24 pagineOxygenation and Airway Management: Quick LookNining Komala SariNessuna valutazione finora
- Pleura: LungsDocumento7 paginePleura: LungsbarbacumlaudeNessuna valutazione finora
- Dissertation On Copd - by - Shivbalak (2013)Documento108 pagineDissertation On Copd - by - Shivbalak (2013)ShivBalakChauhanNessuna valutazione finora
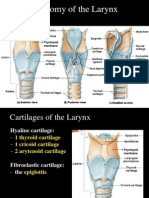
- Anatomy of The Larynx: Thyrohyoid MembraneDocumento35 pagineAnatomy of The Larynx: Thyrohyoid MembraneVarsha Shende KhobragadeNessuna valutazione finora
- GC Proceedings - Docx1Documento11 pagineGC Proceedings - Docx1Thejus BhaskarNessuna valutazione finora
- OxygenationDocumento20 pagineOxygenationKhie-An OcampoNessuna valutazione finora
- Anatomy Ii: by Dr. Ziyad M. Al Zeer Orthopedic Surgeon Assistant Professor MD - PHDDocumento64 pagineAnatomy Ii: by Dr. Ziyad M. Al Zeer Orthopedic Surgeon Assistant Professor MD - PHDMOHAMMAD ALSWEITYNessuna valutazione finora
- Clinical Anatomy of Respiratory System: Dr. Ridwan Harrianto MHSC (Om), SP - OkDocumento31 pagineClinical Anatomy of Respiratory System: Dr. Ridwan Harrianto MHSC (Om), SP - OkMahasiswa StrugleNessuna valutazione finora
- Respiratory Physiology & AnesthesiaDocumento47 pagineRespiratory Physiology & AnesthesiaWenny Eka FildayantiNessuna valutazione finora
- Bolu Seminar in Lungs 2Documento34 pagineBolu Seminar in Lungs 2Bamgbose OpeyemiNessuna valutazione finora
- 10.1. Chest ExaminationDocumento101 pagine10.1. Chest Examinationmirabel IvanaliNessuna valutazione finora
- Class 1 ED (Pneumothorax Paper)Documento31 pagineClass 1 ED (Pneumothorax Paper)Shafiq KadirNessuna valutazione finora
- Assignment On Chest PhysiotherapyDocumento15 pagineAssignment On Chest PhysiotherapyAxsa AlexNessuna valutazione finora
- Chest X-Ray Interpretation: Bucky Boaz, ARNP-CDocumento101 pagineChest X-Ray Interpretation: Bucky Boaz, ARNP-CAnna DiaconuNessuna valutazione finora
- Breathe Easy: Relieving the Symptoms of Chronic Lung DiseaseDa EverandBreathe Easy: Relieving the Symptoms of Chronic Lung DiseaseNessuna valutazione finora
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesDa EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNessuna valutazione finora
- Weight Loss Military UsDocumento277 pagineWeight Loss Military UsGregory JamesNessuna valutazione finora
- Cervical Spine Injury GregDocumento49 pagineCervical Spine Injury GregGregory JamesNessuna valutazione finora
- Digital Nerve BlockDocumento5 pagineDigital Nerve BlockGregory JamesNessuna valutazione finora
- Cme Acute AbdomenDocumento110 pagineCme Acute AbdomenGregory JamesNessuna valutazione finora
- Research ArticleDocumento10 pagineResearch ArticleGregory JamesNessuna valutazione finora
- Daftar PustakaDocumento1 paginaDaftar PustakaGregory JamesNessuna valutazione finora
- Rig SandhyavandanamDocumento39 pagineRig Sandhyavandanamhgiri2007Nessuna valutazione finora
- Avian Skeletal System - Robert Porter PDFDocumento16 pagineAvian Skeletal System - Robert Porter PDFJohn MillerNessuna valutazione finora
- Consultation, Medical History and Record TakingDocumento19 pagineConsultation, Medical History and Record TakingdmorcfNessuna valutazione finora
- Kode Simpus PTT EMIDocumento18 pagineKode Simpus PTT EMIfauziahNessuna valutazione finora
- Chronic OsteomyelitisDocumento58 pagineChronic OsteomyelitisSumukha RajeshNessuna valutazione finora
- Labanotation and Life Forms - ICKL - International Council of (PDFDrive)Documento12 pagineLabanotation and Life Forms - ICKL - International Council of (PDFDrive)Aryon KnightNessuna valutazione finora
- Mastectomy and Physiotherapy Management Final YearDocumento24 pagineMastectomy and Physiotherapy Management Final YearNithin Nair57% (7)
- Thorax 1Documento10 pagineThorax 1Khushi ShahNessuna valutazione finora
- Parts of The Body: Teacher: Miss Nataly Oñate GDocumento8 pagineParts of The Body: Teacher: Miss Nataly Oñate Gcarmen gloriaNessuna valutazione finora
- Human Anatomy,: Chapter 13 Lecture Outline: Surface AnatomyDocumento57 pagineHuman Anatomy,: Chapter 13 Lecture Outline: Surface AnatomyLavina SofiaNessuna valutazione finora
- Superior Sulcus (Pancoast) Tumors Current Evidence On Diagnosis and Radical TreanmentDocumento17 pagineSuperior Sulcus (Pancoast) Tumors Current Evidence On Diagnosis and Radical TreanmentAnwar JallingNessuna valutazione finora
- 101 Chest X Ray Solutions 2013Documento281 pagine101 Chest X Ray Solutions 2013Mohamed Saeed El Khayat100% (4)
- The Lazy Mans Guide To RelaxationDocumento84 pagineThe Lazy Mans Guide To Relaxationssm0% (1)
- Manitou Telehandler MT 14 To 18 M Repair ManualDocumento23 pagineManitou Telehandler MT 14 To 18 M Repair Manualmscassandravasquez120985pgc100% (111)
- Anathomy AtlasDocumento22 pagineAnathomy AtlasBogdan SoltuzuNessuna valutazione finora
- Qi GongDocumento13 pagineQi GongMarcus Ramos100% (3)
- Attorney General's Report On Death of Jaime Lopez-CabreraDocumento65 pagineAttorney General's Report On Death of Jaime Lopez-CabreraAnonymous okrJR6rTRNessuna valutazione finora
- Good Posture in SingingDocumento2 pagineGood Posture in SinginghyrdaNessuna valutazione finora
- Massage 101Documento33 pagineMassage 101Vladislav KotovNessuna valutazione finora
- Body Scan ScriptDocumento10 pagineBody Scan Scriptmike9and100% (1)
- Pelvic Floor Awareness For Psychosexual TherapyDocumento8 paginePelvic Floor Awareness For Psychosexual Therapy842janxNessuna valutazione finora
- Hartman 1966 Polychaeta Sedentaria Antarctica LiteDocumento166 pagineHartman 1966 Polychaeta Sedentaria Antarctica LiteValentina Sandoval ParraNessuna valutazione finora
- Luka Bakar Morning ReportDocumento24 pagineLuka Bakar Morning ReportUmmatul KhairiyahNessuna valutazione finora
- Gaseous Exchange Grade 11Documento38 pagineGaseous Exchange Grade 11ThatoNessuna valutazione finora
- Chest TraumaDocumento115 pagineChest TraumaЕвгений ХанькоNessuna valutazione finora
- Bates' Guide To Physical Examination and History Taking, 12th EditionDocumento9 pagineBates' Guide To Physical Examination and History Taking, 12th Editionmanes0% (1)
- Badminton Coaching 2016Documento32 pagineBadminton Coaching 2016dennis sabornidoNessuna valutazione finora
- ABS-Anatomy of The ThoraxDocumento52 pagineABS-Anatomy of The ThoraxAtti Tamas100% (1)
- Breathing TechniquesDocumento26 pagineBreathing TechniquessherryNessuna valutazione finora
- Managing COVID at HomeDocumento24 pagineManaging COVID at HomeShumaila MirzaNessuna valutazione finora