Potrebbero piacerti anche
- Biophysical Characterization of Dry Facial Skin: J. L. Leveque, G. Grove, J. de Rigal, P. CorcuffDocumento8 pagineBiophysical Characterization of Dry Facial Skin: J. L. Leveque, G. Grove, J. de Rigal, P. CorcuffLanna HarumiyaNessuna valutazione finora
- 10 0000@Www Jstage JST Go jp@Article@Jat@23@11@2335436@ArticleDocumento9 pagine10 0000@Www Jstage JST Go jp@Article@Jat@23@11@2335436@ArticleLanna HarumiyaNessuna valutazione finora
- Gloomy LifeDocumento6 pagineGloomy LifeLanna HarumiyaNessuna valutazione finora
- Click To Edit Master Subtitle StyleDocumento4 pagineClick To Edit Master Subtitle StyleLanna HarumiyaNessuna valutazione finora
- Click To Edit Master Subtitle StyleDocumento4 pagineClick To Edit Master Subtitle StyleLanna HarumiyaNessuna valutazione finora
- Presentation TitleDocumento4 paginePresentation TitleLanna HarumiyaNessuna valutazione finora
- Click To Edit Master Title StyleDocumento4 pagineClick To Edit Master Title StyleLanna HarumiyaNessuna valutazione finora
- Kol Ditz 2016Documento3 pagineKol Ditz 2016Lanna HarumiyaNessuna valutazione finora
- Tentative Acara Workshop SimpoDocumento7 pagineTentative Acara Workshop SimpoLanna HarumiyaNessuna valutazione finora
- Title: SubheadingDocumento7 pagineTitle: SubheadingLanna HarumiyaNessuna valutazione finora
- Frans Sarumpaet, Dr. Pembimbing: Bayu Rusfandi, DR., SPPDDocumento13 pagineFrans Sarumpaet, Dr. Pembimbing: Bayu Rusfandi, DR., SPPDLanna HarumiyaNessuna valutazione finora
- Related InfectionDocumento3 pagineRelated InfectionLanna HarumiyaNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Diseases, Ailments, and Disorders in Urinary System - PPTDocumento24 pagineDiseases, Ailments, and Disorders in Urinary System - PPTIsabella Alycia Lomibao100% (1)
- BIRADS Poster 36x24in FDocumento1 paginaBIRADS Poster 36x24in FBk Del Riego100% (1)
- In Silico Molecular Docking of Marine Drugs Against Cancer ProteinsDocumento5 pagineIn Silico Molecular Docking of Marine Drugs Against Cancer ProteinsSEP-PublisherNessuna valutazione finora
- Vasculitis RoadmapDocumento117 pagineVasculitis Roadmapdockamag100% (1)
- Lets Talk About Health Fun Activities Games Oneonone Activities Pronuncia - 1996Documento1 paginaLets Talk About Health Fun Activities Games Oneonone Activities Pronuncia - 1996jadransko moreNessuna valutazione finora
- Master Oral MedicineDocumento54 pagineMaster Oral MedicineDr. MujahidNessuna valutazione finora
- hnf41 Revised by Lau - To Be PrintDocumento62 paginehnf41 Revised by Lau - To Be PrintJessa EsguerraNessuna valutazione finora
- European Heart JournalDocumento50 pagineEuropean Heart JournalAgustin CNessuna valutazione finora
- Chapter 21 DigestionDocumento96 pagineChapter 21 DigestionJwnsbdhdNessuna valutazione finora
- Irfan Mir NotesDocumento199 pagineIrfan Mir NotesSwathi AnantulaNessuna valutazione finora
- How To Make Your Own Colloidal SilverDocumento21 pagineHow To Make Your Own Colloidal Silverrawzero92% (12)
- Crimes of The Century: Occupation & Contaminating Iraq With Depleted UraniumDocumento28 pagineCrimes of The Century: Occupation & Contaminating Iraq With Depleted Uraniumpaola pisiNessuna valutazione finora
- The Budwig DietDocumento3 pagineThe Budwig DietANGELO NHARNessuna valutazione finora
- Biopsy in Surgery RereDocumento41 pagineBiopsy in Surgery RereRererloluwa100% (1)
- Oncocytoma of The Nasal CavityDocumento2 pagineOncocytoma of The Nasal CavityInes Camilla PutriNessuna valutazione finora
- SinusitisDocumento402 pagineSinusitisIsidro Roberto Santana Gonzalez100% (1)
- DrugsDocumento5 pagineDrugsdeepika kushwah100% (1)
- Pasteurelosis Neumónica (Mannheimiosis) BovinaDocumento22 paginePasteurelosis Neumónica (Mannheimiosis) BovinaJesus Bustillo0% (1)
- PancreatitisDocumento59 paginePancreatitisAarif RanaNessuna valutazione finora
- Ovarian Cancer: PathophysiologyDocumento3 pagineOvarian Cancer: PathophysiologyXarius FidelNessuna valutazione finora
- Cat 2009 para JumbledDocumento2 pagineCat 2009 para JumbledmymentorpalasiaNessuna valutazione finora
- Functional Gastrointestinal DisordersDocumento126 pagineFunctional Gastrointestinal DisordersCri Cristiana100% (1)
- CPG Management of Breast Cancer (2nd Edition) 2010 PDFDocumento100 pagineCPG Management of Breast Cancer (2nd Edition) 2010 PDFNana Nurliana NoorNessuna valutazione finora
- Thyroid Gland NotesDocumento21 pagineThyroid Gland NotesbryanNessuna valutazione finora
- Pcod SonogramDocumento1 paginaPcod SonogramsanjanaNessuna valutazione finora
- BIOL 2210 Chapter 6, Integument System-1Documento15 pagineBIOL 2210 Chapter 6, Integument System-1KellyPatrick SpencerNessuna valutazione finora
- 1a) III) Importance of MTBEDocumento4 pagine1a) III) Importance of MTBEMuhammad HaikalNessuna valutazione finora
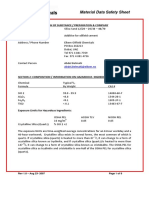
- Silica Sand MSDSDocumento8 pagineSilica Sand MSDSizzybjNessuna valutazione finora
- Application of Radiotracer in MedicineDocumento17 pagineApplication of Radiotracer in MedicineUsama NazeerNessuna valutazione finora
- Urine SedimentDocumento38 pagineUrine Sedimentcyrhenmie100% (1)