Potrebbero piacerti anche
- Heavy Metal Intoxication and Chelators MCQ Answer SheetDocumento4 pagineHeavy Metal Intoxication and Chelators MCQ Answer SheetPatrick Dycoco75% (4)
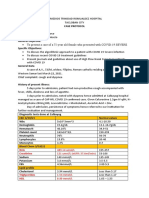
- Case Protocol Covid SevereDocumento3 pagineCase Protocol Covid SeverePatrick DycocoNessuna valutazione finora
- Approach To Liver HH (Autosaved)Documento59 pagineApproach To Liver HH (Autosaved)Patrick Dycoco100% (1)
- EVRMC 1st EndorsementDocumento4 pagineEVRMC 1st EndorsementPatrick DycocoNessuna valutazione finora
- History Taking 3Documento4 pagineHistory Taking 3Patrick DycocoNessuna valutazione finora
- Cerebral PerfusionDocumento5 pagineCerebral PerfusionPatrick DycocoNessuna valutazione finora
- Case Study - BlenteDocumento10 pagineCase Study - BlentePatrick DycocoNessuna valutazione finora
- CHFDocumento7 pagineCHFPatrick DycocoNessuna valutazione finora
- Related Lit Additional (Mercado)Documento7 pagineRelated Lit Additional (Mercado)Patrick DycocoNessuna valutazione finora
- Spot Map Part 1Documento1 paginaSpot Map Part 1Patrick DycocoNessuna valutazione finora
- PCM Epidemiology of Yellow FeverDocumento7 paginePCM Epidemiology of Yellow FeverPatrick DycocoNessuna valutazione finora
- Spot Map Part 1Documento1 paginaSpot Map Part 1Patrick DycocoNessuna valutazione finora
- Dengue Pedia MMCDocumento26 pagineDengue Pedia MMCPatrick DycocoNessuna valutazione finora
- Dengue Pedia MMCDocumento26 pagineDengue Pedia MMCPatrick DycocoNessuna valutazione finora
- STDDocumento69 pagineSTDPatrick DycocoNessuna valutazione finora
- IntussusceptionDocumento10 pagineIntussusceptionPatrick DycocoNessuna valutazione finora
- AsthmaDocumento72 pagineAsthmaPatrick DycocoNessuna valutazione finora
- Gugon, Pcap DDocumento6 pagineGugon, Pcap DPatrick DycocoNessuna valutazione finora
- Acute GastroenteritisDocumento4 pagineAcute GastroenteritisPatrick DycocoNessuna valutazione finora
- Tetralogy of Fallot with Hypercyanotic SpellsDocumento11 pagineTetralogy of Fallot with Hypercyanotic SpellsPatrick DycocoNessuna valutazione finora
- Acute PancreatitisDocumento7 pagineAcute PancreatitisPatrick DycocoNessuna valutazione finora
- TofDocumento5 pagineTofPatrick DycocoNessuna valutazione finora
- Review of SystemsDocumento2 pagineReview of SystemsPatrick DycocoNessuna valutazione finora
- Difficulty Breathing Patient InterviewDocumento1 paginaDifficulty Breathing Patient InterviewPatrick DycocoNessuna valutazione finora
- PCM Epidemiology of Yellow FeverDocumento7 paginePCM Epidemiology of Yellow FeverPatrick DycocoNessuna valutazione finora
- Superficial MycosesDocumento6 pagineSuperficial MycosesPatrick DycocoNessuna valutazione finora
- SeizureDocumento7 pagineSeizurePatrick DycocoNessuna valutazione finora
- Blood Supply of Head and NeckDocumento44 pagineBlood Supply of Head and NeckPatrick DycocoNessuna valutazione finora
- Distance & Speed ProblemsDocumento2 pagineDistance & Speed ProblemsAnonymous GNWnQacNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Vangsness2009 GlucosamineDocumento9 pagineVangsness2009 GlucosaminebuddybbuddyNessuna valutazione finora
- Implementing Guidelines for Health Discounts and Privileges for PWDsDocumento11 pagineImplementing Guidelines for Health Discounts and Privileges for PWDsjeffrey arzagaNessuna valutazione finora
- Paper On Intergenerational TraumaDocumento13 paginePaper On Intergenerational TraumaEdith G.LebelNessuna valutazione finora
- DrugsDocumento17 pagineDrugsQais ShaikhNessuna valutazione finora
- Chocolate Milk Argument Essay SamplesDocumento3 pagineChocolate Milk Argument Essay Samplesapi-349881433100% (4)
- PenicillinDocumento75 paginePenicillinJean CabigaoNessuna valutazione finora
- Prepare Sponge and CakesDocumento30 paginePrepare Sponge and Cakesmarilyn rosilNessuna valutazione finora
- CrohnsDocumento19 pagineCrohnsLauren LevyNessuna valutazione finora
- Ohi Graphic OrganizerDocumento1 paginaOhi Graphic Organizerapi-278298083Nessuna valutazione finora
- Digestive Disorders April 2007 PDFDocumento8 pagineDigestive Disorders April 2007 PDFAnanta RanaNessuna valutazione finora
- Teaching Plan On Newborn ScreeningDocumento8 pagineTeaching Plan On Newborn ScreeningQueenie Sicco100% (1)
- Birštonas Toursim Manual 2022Documento64 pagineBirštonas Toursim Manual 2022Visit BirštonasNessuna valutazione finora
- IMPLANT OCCLUSION GUIDEDocumento57 pagineIMPLANT OCCLUSION GUIDEElango2548994% (16)
- Pain Management: Dr. Surya Bayu Prajayana, M.Biomed, Sp. OTDocumento22 paginePain Management: Dr. Surya Bayu Prajayana, M.Biomed, Sp. OTOgizWaraNessuna valutazione finora
- EVOLUTION OF CARD REPERTORYDocumento7 pagineEVOLUTION OF CARD REPERTORYRahul RamanNessuna valutazione finora
- Narcotics Anonymous Meeting 3Documento6 pagineNarcotics Anonymous Meeting 3api-401390929Nessuna valutazione finora
- CPT ChecklistDocumento1 paginaCPT ChecklistphilippepreanNessuna valutazione finora
- 1 - O - Anuruddha KumaraDocumento8 pagine1 - O - Anuruddha Kumaraumapati 1505Nessuna valutazione finora
- Anxiety DisorderDocumento9 pagineAnxiety DisorderSatish KujurNessuna valutazione finora
- RN review nuggets: Essential fundamentals of nursingDocumento32 pagineRN review nuggets: Essential fundamentals of nursingr.a.g.Nessuna valutazione finora
- Postpartum HaemorrhageDocumento19 paginePostpartum HaemorrhageJonas Marvin AnaqueNessuna valutazione finora
- COR PULMONALE - MahasiswaDocumento14 pagineCOR PULMONALE - MahasiswaGalih Maygananda PutraNessuna valutazione finora
- Psychology Presentation Chapter 10 - Life Span DevelopmentDocumento15 paginePsychology Presentation Chapter 10 - Life Span DevelopmentEduardo VillanuevaNessuna valutazione finora
- Classroom Lesson PlansDocumento34 pagineClassroom Lesson PlansZakia Aikaz100% (1)
- GDC Dental Team WorkingDocumento12 pagineGDC Dental Team WorkingRamona RochianNessuna valutazione finora
- DisolusiDocumento47 pagineDisolusiNoonaNuzha Lestary NuzhaAyuNessuna valutazione finora
- Reverse AlzheimersDocumento40 pagineReverse Alzheimersakajhon100% (9)
- Female Welfare ProgrammeDocumento6 pagineFemale Welfare ProgrammeAnnapurna DangetiNessuna valutazione finora
- Transcatheter EmbolizationDocumento9 pagineTranscatheter EmbolizationPatrick SalengaNessuna valutazione finora
- AmenorrheaDocumento41 pagineAmenorrheaDewi Felayati Gusni100% (2)