Potrebbero piacerti anche
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- CH 5 SaladinDocumento95 pagineCH 5 Saladinalphabennydelta4468100% (1)
- Calbiochem InhibitorsDocumento124 pagineCalbiochem InhibitorsChazMarloweNessuna valutazione finora
- Human CloningDocumento2 pagineHuman Cloningapi-318868666Nessuna valutazione finora
- Molecular Networking As A Drug Discovery, Drug Metabolism, and Precision Medicine StrategyDocumento12 pagineMolecular Networking As A Drug Discovery, Drug Metabolism, and Precision Medicine StrategySam SonNessuna valutazione finora
- WJCC 8 1172Documento13 pagineWJCC 8 1172johoba5344Nessuna valutazione finora
- Submerged Cultivation of Medicinal MushroomsDocumento30 pagineSubmerged Cultivation of Medicinal Mushroomsbravohr98Nessuna valutazione finora
- PCR 5 Lab SetupDocumento22 paginePCR 5 Lab Setupptz1965Nessuna valutazione finora
- Movement Disorders Movement DisordersDocumento32 pagineMovement Disorders Movement Disordersreddyrajiv1526Nessuna valutazione finora
- Chronic Condition Self-Management Approaches Research and EvaluationDocumento50 pagineChronic Condition Self-Management Approaches Research and EvaluationFakir TajulNessuna valutazione finora
- Biol 460 Case StudyDocumento11 pagineBiol 460 Case Studyapi-353888678Nessuna valutazione finora
- FHSC1234 Tutorial 9S 202210Documento5 pagineFHSC1234 Tutorial 9S 202210Zhi YongNessuna valutazione finora
- Spatial Transcriptomics Reveals Distinct and Conserved Tumor Core and Edge Architectures That Predict Survival and Targeted Therapy ResponseDocumento61 pagineSpatial Transcriptomics Reveals Distinct and Conserved Tumor Core and Edge Architectures That Predict Survival and Targeted Therapy Response戴义宾Nessuna valutazione finora
- Hille B-Second Edition (For Printing)Documento617 pagineHille B-Second Edition (For Printing)matuskacarlosNessuna valutazione finora
- Molecular Detection of Extended Spectrum B-Lactamases, MetalloDocumento7 pagineMolecular Detection of Extended Spectrum B-Lactamases, MetalloValentina RondonNessuna valutazione finora
- Coccidia 10 - 11Documento40 pagineCoccidia 10 - 11microperadeniya100% (1)
- Muscular SystemDocumento20 pagineMuscular SystemAltaf Hussain KhanNessuna valutazione finora
- 1.1 Fields and Careers in BiologyDocumento5 pagine1.1 Fields and Careers in BiologyFHATIN AMIRA BINTI MUSA MoeNessuna valutazione finora
- The Thalassemias and Hemolytic AnemiasDocumento43 pagineThe Thalassemias and Hemolytic AnemiasAnonymous elq7jZiSNessuna valutazione finora
- Treatment of Differentiated Thyroid Cancers with Tyrosine Kinase InhibitorsDocumento28 pagineTreatment of Differentiated Thyroid Cancers with Tyrosine Kinase InhibitorsSameer FasihNessuna valutazione finora
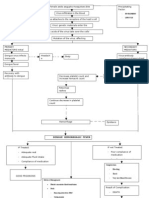
- Pathophysio DHF EDITEDDocumento3 paginePathophysio DHF EDITEDricmichael100% (1)
- Criminal Behavior Genre DraftDocumento6 pagineCriminal Behavior Genre Draftapi-309159739Nessuna valutazione finora
- Cellular Nutrition - The Key to Preventing Oxidative StressDocumento4 pagineCellular Nutrition - The Key to Preventing Oxidative StressFxStuntDriver100% (3)
- Current GM Crops & Transgenic AnimalsDocumento12 pagineCurrent GM Crops & Transgenic AnimalsJhayce Christian S. CapanayanNessuna valutazione finora
- Bioactive Natural Products Opportunities and Challenges in MedicinalDocumento695 pagineBioactive Natural Products Opportunities and Challenges in Medicinalney.barbosaNessuna valutazione finora
- Improving Eyesight With Red Light TherapyDocumento23 pagineImproving Eyesight With Red Light TherapyMark Sloan100% (8)
- Nocturnal EnuresisDocumento38 pagineNocturnal EnuresisayshuyNessuna valutazione finora
- Lessons Learned From The Gene Therapy Trial For OrnithineDocumento7 pagineLessons Learned From The Gene Therapy Trial For OrnithineAfifa ZeeshanNessuna valutazione finora
- Bacterial Conjugation Programming - Jimmy VenturaDocumento5 pagineBacterial Conjugation Programming - Jimmy VenturaJimmy VenturaNessuna valutazione finora
- NCP For Ectopic PregnancyDocumento4 pagineNCP For Ectopic PregnancyClarissa_Dante_735850% (4)