Potrebbero piacerti anche
- GUIDEBOOK To Clinical Optometry Internship 2016Documento77 pagineGUIDEBOOK To Clinical Optometry Internship 2016Marjune Dimayuga100% (3)
- BridgeSpan Speech Services Guidelines - V102019 - Eff03012019 - Pub10222018 PDFDocumento245 pagineBridgeSpan Speech Services Guidelines - V102019 - Eff03012019 - Pub10222018 PDFMariel Salazar100% (2)
- Obesity GuidelinesDocumento232 pagineObesity GuidelinesLORES14100% (1)
- Nicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFDocumento927 pagineNicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFJamie Baczewski100% (8)
- Stroke Thrombectomy Mentored Implementation ProgramDocumento63 pagineStroke Thrombectomy Mentored Implementation ProgramAnonymous NIPCTC68xiNessuna valutazione finora
- 2 - What To Use Colloidal Silver For-2016Documento24 pagine2 - What To Use Colloidal Silver For-2016AB236100% (1)
- Textbook of Reumathology-Kelley's PDFDocumento1.909 pagineTextbook of Reumathology-Kelley's PDFFlorentina Sterghiu100% (4)
- NCM 119 Module Safety Part 2 Standards Lesson Safety National Quality Forum 2009Documento59 pagineNCM 119 Module Safety Part 2 Standards Lesson Safety National Quality Forum 2009Maria Victoria A. PraxidesNessuna valutazione finora
- Thyroid Disease in PregnancyDocumento36 pagineThyroid Disease in Pregnancypeni_dwiNessuna valutazione finora
- Patient Engagement: Technical Series On Safer Primary CareDocumento26 paginePatient Engagement: Technical Series On Safer Primary CareHndrNessuna valutazione finora
- Infection Control NHS PolicyDocumento12 pagineInfection Control NHS PolicyYahya Salem100% (1)
- CMO No 25 Series 2021 PSG For BS PharmacyDocumento49 pagineCMO No 25 Series 2021 PSG For BS PharmacyIrenelle OdtojanNessuna valutazione finora
- Clinical Pathways and Nurses.Documento3 pagineClinical Pathways and Nurses.Natukunda Dianah100% (1)
- The Management of Keloids and Hypertrophic ScarsDocumento7 pagineThe Management of Keloids and Hypertrophic Scarsdonlot lover100% (1)
- Manajemen HospitalDocumento28 pagineManajemen HospitalDike Widyakti Sawfina MaharaniNessuna valutazione finora
- Infection Control Program in The HospitalDocumento14 pagineInfection Control Program in The HospitalLorelie Asis100% (1)
- Congenital HypothyroidismDocumento2 pagineCongenital Hypothyroidismapi-321672273Nessuna valutazione finora
- Impaired MemoryDocumento1 paginaImpaired MemoryHarmony Grace0% (1)
- Process Evaluation of A National Primary Eye Care Programme in RwandaDocumento12 pagineProcess Evaluation of A National Primary Eye Care Programme in RwandaEvan McCartneyNessuna valutazione finora
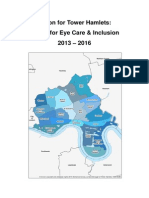
- Tower Hamlets Plan For EyecareDocumento47 pagineTower Hamlets Plan For EyecarevmoschasNessuna valutazione finora
- WCO Position Statement On The World Report On Vision July 2022Documento3 pagineWCO Position Statement On The World Report On Vision July 2022Eunice DichosoNessuna valutazione finora
- Who Uhl Technical Brief VisionDocumento4 pagineWho Uhl Technical Brief VisionVenice ReyesNessuna valutazione finora
- Article by DR Arvind Kumar MoryaDocumento3 pagineArticle by DR Arvind Kumar MoryaSulabh Sahu100% (2)
- OphthalmologyDocumento69 pagineOphthalmologyjatavNessuna valutazione finora
- Integrated Care PathwayDocumento3 pagineIntegrated Care PathwayFitri EmiNessuna valutazione finora
- Organize Care Around Medical Conditions - Institute For Strategy and Competitiveness - Harvard Business SchoolDocumento3 pagineOrganize Care Around Medical Conditions - Institute For Strategy and Competitiveness - Harvard Business SchoolTuan Nguyen DangNessuna valutazione finora
- Eye Care ReportDocumento20 pagineEye Care ReportJoeven HilarioNessuna valutazione finora
- ASE ModelDocumento12 pagineASE Modellolmimi0100Nessuna valutazione finora
- Study Guide 5: Evidence-Based Practices in Nursing Management Topic OutlineDocumento4 pagineStudy Guide 5: Evidence-Based Practices in Nursing Management Topic OutlineElizabeth DaligdigNessuna valutazione finora
- To Become The World's Best Tertiary Healthcare ProviderDocumento13 pagineTo Become The World's Best Tertiary Healthcare ProviderShah BrijeshkumarNessuna valutazione finora
- Technology Guidelines For A District Eye Care Programme: July 2006Documento53 pagineTechnology Guidelines For A District Eye Care Programme: July 2006Peter AbikoyeNessuna valutazione finora
- The Cost of CareDocumento3 pagineThe Cost of CareSpeech & Language Therapy in PracticeNessuna valutazione finora
- Innovation Awards Round 2 Batch 1Documento7 pagineInnovation Awards Round 2 Batch 1iggybauNessuna valutazione finora
- Guide For Developing AWHSC Patient Safety Policy and Strategic PlanDocumento17 pagineGuide For Developing AWHSC Patient Safety Policy and Strategic PlanAddis YeshitlaNessuna valutazione finora
- 1.1. Eye - & - Vision - Care - Toolkit - HOW-TO-GUIDEDocumento16 pagine1.1. Eye - & - Vision - Care - Toolkit - HOW-TO-GUIDECynthia Jaramillo MachucaNessuna valutazione finora
- 2.07-4.6 Global Fund Strategic Approach To HSS. WHO ReportDocumento50 pagine2.07-4.6 Global Fund Strategic Approach To HSS. WHO ReportGeorge KorahNessuna valutazione finora
- Commentary: Ophthalmic Increasing Operations ofDocumento2 pagineCommentary: Ophthalmic Increasing Operations ofDurval SantosNessuna valutazione finora
- Code Grey Standards - May 2014 PDFDocumento3 pagineCode Grey Standards - May 2014 PDFmaharaniNessuna valutazione finora
- Training Standards in Implant Dentistry 2016Documento13 pagineTraining Standards in Implant Dentistry 2016Ramona RochianNessuna valutazione finora
- Draft UHC Pilot Project ProposalDocumento19 pagineDraft UHC Pilot Project ProposalNanditha ChowhanNessuna valutazione finora
- Who Disability-Inclusive Health Services Training PackageDocumento106 pagineWho Disability-Inclusive Health Services Training PackageAz-Zahraa NaasNessuna valutazione finora
- Equip Second ManualDocumento76 pagineEquip Second ManualArjun SutharNessuna valutazione finora
- South Africa EHealth Strategy 2012 2017Documento36 pagineSouth Africa EHealth Strategy 2012 2017calderon5736Nessuna valutazione finora
- National Telemedicine Guidelines For SingaporeDocumento41 pagineNational Telemedicine Guidelines For SingaporeNakul Singh ParkwayIndiaNessuna valutazione finora
- Why OptometryDocumento30 pagineWhy OptometrysandiNessuna valutazione finora
- Jmid 4 Mitp FinalDocumento21 pagineJmid 4 Mitp FinalJose Ignacio ZalbaNessuna valutazione finora
- Kuwait Declaration On Patient SafetyDocumento5 pagineKuwait Declaration On Patient Safetyanita astaliaNessuna valutazione finora
- The Contribution of Technology AssessmentDocumento11 pagineThe Contribution of Technology AssessmentFirmansyah LabanuNessuna valutazione finora
- Epidemiology and Community OptometryDocumento3 pagineEpidemiology and Community OptometrySayoki GhoshNessuna valutazione finora
- Producing Competent Physicians - More Paper Work or IndeedDocumento48 pagineProducing Competent Physicians - More Paper Work or Indeedapi-26176346Nessuna valutazione finora
- VIP Documentary Script Revised+n Edits RevisedDocumento4 pagineVIP Documentary Script Revised+n Edits RevisedRael GibendiNessuna valutazione finora
- Policy Brief: Strengthening Human Resources For Eye Health in SADC CountriesDocumento2 paginePolicy Brief: Strengthening Human Resources For Eye Health in SADC CountriesHelpAge InternationalNessuna valutazione finora
- Core Resilientsustainablesystemsforhealth Infonote enDocumento35 pagineCore Resilientsustainablesystemsforhealth Infonote enSponge BobNessuna valutazione finora
- Health Systems: Aurthor (S)Documento6 pagineHealth Systems: Aurthor (S)Sucheta MitraNessuna valutazione finora
- Dr. Bu Castro PHAPi-ANC Presentation-11.18.19Documento40 pagineDr. Bu Castro PHAPi-ANC Presentation-11.18.19Arah Obias CopeNessuna valutazione finora
- 2005 PROF 018 OphthalmicPrimaryCare2005Documento7 pagine2005 PROF 018 OphthalmicPrimaryCare2005Annisa KhairunnisaNessuna valutazione finora
- New Technologies On Public Health: Dr. Judith J. Sugay Faculty, Feu-InDocumento23 pagineNew Technologies On Public Health: Dr. Judith J. Sugay Faculty, Feu-InBianca SandovalNessuna valutazione finora
- Roadmap For Personalized Health Care April 2011Documento8 pagineRoadmap For Personalized Health Care April 2011divith3010Nessuna valutazione finora
- Public Health OphthalmologyDocumento52 paginePublic Health OphthalmologyunonounoNessuna valutazione finora
- Infection Control Protocols in Specialist Dental Centre at Saudi Arabia. A NewappresialDocumento6 pagineInfection Control Protocols in Specialist Dental Centre at Saudi Arabia. A NewappresialIJAR JOURNALNessuna valutazione finora
- Evaluation of Telemedicine SystemDocumento8 pagineEvaluation of Telemedicine Systemfatma mohammedNessuna valutazione finora
- Health & Wellbeing Topics For Research: OpicsDocumento9 pagineHealth & Wellbeing Topics For Research: Opicsafolea1823Nessuna valutazione finora
- SBIRT BookletDocumento12 pagineSBIRT BookletShannon RaspNessuna valutazione finora
- BUS6004 Quality Management in A Care Setting - EditedDocumento13 pagineBUS6004 Quality Management in A Care Setting - EditedMashaal FNessuna valutazione finora
- Homecare Guidance - 2019Documento19 pagineHomecare Guidance - 2019ahamedsahibNessuna valutazione finora
- Joint Commission Research PaperDocumento8 pagineJoint Commission Research Paperuzypvhhkf100% (1)
- Medication Errors: Technical Series On Safer Primary CareDocumento31 pagineMedication Errors: Technical Series On Safer Primary CaredidikNessuna valutazione finora
- Job Title: Podiatrist Band: 5 Responsible To: Podiatry Clinical Lead Accountable To: Senior Manager Base: Edgware Community Hospital Job PurposeDocumento9 pagineJob Title: Podiatrist Band: 5 Responsible To: Podiatry Clinical Lead Accountable To: Senior Manager Base: Edgware Community Hospital Job PurposeMD Luthfy LubisNessuna valutazione finora
- Construction and Demolition Waste ToolDocumento60 pagineConstruction and Demolition Waste ToolBassam Al-HimiariNessuna valutazione finora
- Plastics Waste ToolDocumento70 paginePlastics Waste ToolBassam Al-HimiariNessuna valutazione finora
- Organic Waste ToolDocumento72 pagineOrganic Waste ToolBassam Al-HimiariNessuna valutazione finora
- Electronic Waste ToolDocumento60 pagineElectronic Waste ToolBassam Al-HimiariNessuna valutazione finora
- Nicu Brochure Stanford ChildrensDocumento8 pagineNicu Brochure Stanford ChildrensBassam Al-HimiariNessuna valutazione finora
- Quality Assurance & ImprovementDocumento8 pagineQuality Assurance & ImprovementBassam Al-HimiariNessuna valutazione finora
- External Assessment of Health ServicesDocumento4 pagineExternal Assessment of Health ServicesBassam Al-HimiariNessuna valutazione finora
- Maintenance of 2 Sinks in Bathroom and Kitchen in MDM Office - Sana'a. Assessment of Sanitation Network in MDM Office - Sana'aDocumento1 paginaMaintenance of 2 Sinks in Bathroom and Kitchen in MDM Office - Sana'a. Assessment of Sanitation Network in MDM Office - Sana'aBassam Al-HimiariNessuna valutazione finora
- Kjo 28 197Documento10 pagineKjo 28 197Bassam Al-HimiariNessuna valutazione finora
- Calendrier 2019: Janvier Fevrier Mars Avril MAI JuinDocumento6 pagineCalendrier 2019: Janvier Fevrier Mars Avril MAI JuinBassam Al-HimiariNessuna valutazione finora
- Completion of Work in MDM Office - AbdraboohDocumento1 paginaCompletion of Work in MDM Office - AbdraboohBassam Al-HimiariNessuna valutazione finora
- ISO 9001 Client GuideDocumento4 pagineISO 9001 Client GuideBassam Al-HimiariNessuna valutazione finora
- Illinois: Driver Licensing Agency Contact InformationDocumento1 paginaIllinois: Driver Licensing Agency Contact InformationBassam Al-HimiariNessuna valutazione finora
- Full-Mouth Adhesive Rehabilitation of A Severely Eroded Dentition: The Three-Step Technique. Part 2Documento17 pagineFull-Mouth Adhesive Rehabilitation of A Severely Eroded Dentition: The Three-Step Technique. Part 2Karina OjedaNessuna valutazione finora
- Letter of ApplicationDocumento4 pagineLetter of Applicationmelai_0123Nessuna valutazione finora
- Chap 1&3Documento51 pagineChap 1&3Lady DanielleNessuna valutazione finora
- Review Question Answers For HIT CH 1Documento5 pagineReview Question Answers For HIT CH 1adam593Nessuna valutazione finora
- Safety and Efficacy of The BNT162b2 MRNA Covid-19 Vaccine Through 6 MonthsDocumento13 pagineSafety and Efficacy of The BNT162b2 MRNA Covid-19 Vaccine Through 6 MonthsChristian GaraffaNessuna valutazione finora
- Martha Rogers, Dorothea Orem, Imogene KingDocumento9 pagineMartha Rogers, Dorothea Orem, Imogene KingCASTRO, ANDREI KARL Z.Nessuna valutazione finora
- ARDSDocumento26 pagineARDSDuratul FahliaNessuna valutazione finora
- 584-Article Text-1678-1-10-20221019Documento7 pagine584-Article Text-1678-1-10-20221019Jenerio PanggabeanNessuna valutazione finora
- Grade 5 - ISSUES-AND-CONCERNS-FOR-HEALTH-SCHOOL-READINESS-OTHER-CONCERNSDocumento2 pagineGrade 5 - ISSUES-AND-CONCERNS-FOR-HEALTH-SCHOOL-READINESS-OTHER-CONCERNSDanny LineNessuna valutazione finora
- Quercetin A Promising Treatment For The Common Cold 2329 8731.1000111Documento3 pagineQuercetin A Promising Treatment For The Common Cold 2329 8731.1000111Sameer SamouaNessuna valutazione finora
- Adedayo Osholowu VisualCV ResumeDocumento5 pagineAdedayo Osholowu VisualCV ResumeAdedayo OsholowuNessuna valutazione finora
- Micro TB Culture: Department of Laboratory MedicineDocumento1 paginaMicro TB Culture: Department of Laboratory MedicineSrinivas maheshwaramNessuna valutazione finora
- Industry Breakdown Episode 2: "Pharmaceuticals"Documento7 pagineIndustry Breakdown Episode 2: "Pharmaceuticals"KAVYA GOYAL PGP 2021-23 BatchNessuna valutazione finora
- mySinusitisCoach - Patient Empowerment in Chronic Rhinosinusitis Using Mobile TechnologyDocumento7 paginemySinusitisCoach - Patient Empowerment in Chronic Rhinosinusitis Using Mobile TechnologyMRMISSYNessuna valutazione finora
- DFCI ITI Dec 6Documento4 pagineDFCI ITI Dec 6Andrea JamieNessuna valutazione finora
- Treatment of Giant Cell Arteritis - UpToDateDocumento26 pagineTreatment of Giant Cell Arteritis - UpToDateBeatriz SilvaNessuna valutazione finora
- Within A Year, Nusantics Has Evolved To Be A Key Shaper of Future Health-Biotechnology in IndonesiaDocumento23 pagineWithin A Year, Nusantics Has Evolved To Be A Key Shaper of Future Health-Biotechnology in IndonesiaGatot SubagyoNessuna valutazione finora
- British Heart Foundation - Sedentary Behavior Evidence BriefingDocumento16 pagineBritish Heart Foundation - Sedentary Behavior Evidence BriefingArpine TavakalyanNessuna valutazione finora
- 2006 Vento Infection and ThalassemiaDocumento8 pagine2006 Vento Infection and ThalassemiarumaishaNessuna valutazione finora
- Diabetes (6. Metas Glucémicas - Estándares de Atención Médica en Diabetes-2022)Documento14 pagineDiabetes (6. Metas Glucémicas - Estándares de Atención Médica en Diabetes-2022)Antony Yamid Bolaños VillarrealNessuna valutazione finora
- Closed Comminutive Fracture Middle Left Clavicle Allman Classification Group IDocumento32 pagineClosed Comminutive Fracture Middle Left Clavicle Allman Classification Group IWilliamtatokieesz Tembokrumahampebenjol-benjolNessuna valutazione finora