Potrebbero piacerti anche
- Etiopathogenesis of DeliriumDocumento36 pagineEtiopathogenesis of DeliriumAarti Gupta100% (1)
- DepressionDocumento16 pagineDepressionLEONARDO ANTONIO CASTILLO ZEGARRA100% (1)
- Mental Health CourseDocumento7 pagineMental Health CourseSheryl ThompsonNessuna valutazione finora
- Degenerative DiseasesDocumento29 pagineDegenerative DiseasesAwang WibisonoNessuna valutazione finora
- Suicide-ICM II 2012Documento11 pagineSuicide-ICM II 2012Joshua ObrienNessuna valutazione finora
- Obsessive Compulsive DisorderDocumento26 pagineObsessive Compulsive DisorderMhaane Desepeda VillanuevaNessuna valutazione finora
- DEPRESSIONDocumento19 pagineDEPRESSIONhazrul100% (1)
- Introduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPDocumento33 pagineIntroduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPSachiko Yosores100% (1)
- Antipsychotics HandoutDocumento25 pagineAntipsychotics HandoutTeddy Kurniady ThaherNessuna valutazione finora
- Post Traumatic Stress Disorder 1Documento8 paginePost Traumatic Stress Disorder 1Shubhranshul DwivediNessuna valutazione finora
- List of DisordersDocumento4 pagineList of DisordersRain Simonette GuanNessuna valutazione finora
- Roadmap to a Psychiatric Residency CareerDocumento21 pagineRoadmap to a Psychiatric Residency Careercatalin_ilie_5Nessuna valutazione finora
- EATING DISORDERS: Note Taking OutlineDocumento6 pagineEATING DISORDERS: Note Taking OutlinePaula GarciaNessuna valutazione finora
- The Mechanisms of Postpartum DepressionDocumento70 pagineThe Mechanisms of Postpartum Depressionazniahsyam8269Nessuna valutazione finora
- Forensic Psychiatry Part1Documento25 pagineForensic Psychiatry Part1JasonNessuna valutazione finora
- ECTDocumento24 pagineECTEdgar ManoodNessuna valutazione finora
- Vascular DementiaDocumento3 pagineVascular DementiaAkhmad Ulil AlbabNessuna valutazione finora
- Anxiety DisordersDocumento70 pagineAnxiety DisordersNishantYadav100% (1)
- PsychosomaticsDocumento56 paginePsychosomaticsrajneesh_shastri10Nessuna valutazione finora
- Personality Disorders PDFDocumento414 paginePersonality Disorders PDFLorina SanduNessuna valutazione finora
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenDa EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNessuna valutazione finora
- Symptom Overreporting and Dissociative Experiences: A Qualitative ReviewDocumento13 pagineSymptom Overreporting and Dissociative Experiences: A Qualitative ReviewKamiNessuna valutazione finora
- SchizopDocumento43 pagineSchizopapi-548578435Nessuna valutazione finora
- Anxiety Disorders: Types, Symptoms, and TreatmentsDocumento62 pagineAnxiety Disorders: Types, Symptoms, and TreatmentsPRHSTNessuna valutazione finora
- Understanding Schizophrenia Symptoms and TreatmentDocumento8 pagineUnderstanding Schizophrenia Symptoms and TreatmentCristian ZuñigaNessuna valutazione finora
- AdhdDocumento92 pagineAdhdNeric Ico MagleoNessuna valutazione finora
- Strasburger Et Al-2015-PsyCh JournalDocumento8 pagineStrasburger Et Al-2015-PsyCh JournalPedro CardosoNessuna valutazione finora
- Notes On PsychiatryDocumento10 pagineNotes On PsychiatryMark VillenaNessuna valutazione finora
- World Psychiatry - October 2013Documento100 pagineWorld Psychiatry - October 2013zokica5Nessuna valutazione finora
- Depression - Let's TalkDocumento9 pagineDepression - Let's TalkThavam RatnaNessuna valutazione finora
- Bringing The Full Power of Science To Bear On: Drug Abuse & AddictionDocumento75 pagineBringing The Full Power of Science To Bear On: Drug Abuse & Addictionmlulu100% (1)
- Samuel J. Knapp, Leon D. Vandecreek - Practical Ethics For Psychologists - A Positive Approach (2005)Documento292 pagineSamuel J. Knapp, Leon D. Vandecreek - Practical Ethics For Psychologists - A Positive Approach (2005)Rüya KOLÇAKNessuna valutazione finora
- PSYCH - PsychosomaticdelasalleDocumento58 paginePSYCH - Psychosomaticdelasalleapi-3856051100% (1)
- Major Depressive Disorder: Assessment, Diagnosis, Planning and InterventionsDocumento25 pagineMajor Depressive Disorder: Assessment, Diagnosis, Planning and InterventionsCath CathNessuna valutazione finora
- Depression in Older PeopleDocumento4 pagineDepression in Older PeopleAlina AlinaNessuna valutazione finora
- Causes and Types of Tremor: A Guide to Trembling and ShakingDocumento64 pagineCauses and Types of Tremor: A Guide to Trembling and Shakingbhushan vichareNessuna valutazione finora
- Somatoform&dissociative Disorders Lesson PlanDocumento12 pagineSomatoform&dissociative Disorders Lesson Planapi-284104206Nessuna valutazione finora
- 1-03 Psychotic Disorders CL v1Documento5 pagine1-03 Psychotic Disorders CL v1Dane Mikhael Calica0% (1)
- Assessing and Treating: Suicidal BehaviorsDocumento24 pagineAssessing and Treating: Suicidal BehaviorsgrinakisNessuna valutazione finora
- Psychotropic-Induced Hyponatremia: A ReviewDocumento9 paginePsychotropic-Induced Hyponatremia: A ReviewJAVED ATHER SIDDIQUINessuna valutazione finora
- Signs and symptoms of mental disorders explainedDocumento60 pagineSigns and symptoms of mental disorders explainedgerrgiytryahoo100% (1)
- LewinsohnDocumento14 pagineLewinsohnFabricio Espinoza GamarraNessuna valutazione finora
- Non-Pharmacological Treatments For Depression in Primary Care - An OverviewDocumento8 pagineNon-Pharmacological Treatments For Depression in Primary Care - An OverviewknowlardNessuna valutazione finora
- MENTAL HEALTH GUIDE YOUTH WORKERSDocumento37 pagineMENTAL HEALTH GUIDE YOUTH WORKERSStacia CunninghamNessuna valutazione finora
- Biopsychosocial ModelDocumento1 paginaBiopsychosocial ModelJames SkinnerNessuna valutazione finora
- Midterm Psych Module 7Documento14 pagineMidterm Psych Module 7Ladybelle GototosNessuna valutazione finora
- 1.03 Psychia - The MindDocumento4 pagine1.03 Psychia - The MindDETECTIVE CONANNessuna valutazione finora
- Alzheimers Disease Final PaperDocumento13 pagineAlzheimers Disease Final Paperapi-337834742Nessuna valutazione finora
- Schizoaffective Disorder FactsheetDocumento6 pagineSchizoaffective Disorder FactsheetYusnida RahmawatiNessuna valutazione finora
- Mood DisordersDocumento25 pagineMood DisordersRence IremedioNessuna valutazione finora
- Test Manual Helps Measure Manual DexterityDocumento18 pagineTest Manual Helps Measure Manual DexterityCarlos Andrés NeyraNessuna valutazione finora
- Dementia & DeliriumDocumento7 pagineDementia & DeliriumSudesna Roy ChowdhuryNessuna valutazione finora
- H.4 Borderline PowerPoint Revised 2015Documento31 pagineH.4 Borderline PowerPoint Revised 2015Ptrc Lbr LpNessuna valutazione finora
- Group 4: Courtney Morgan Tyrone NelsonDocumento50 pagineGroup 4: Courtney Morgan Tyrone NelsonTrevannie EdwardsNessuna valutazione finora
- Activities of Daily Living in Patients With Dementia - Clinical Relevance, Methods of Assessment and Effects of TreatmentDocumento23 pagineActivities of Daily Living in Patients With Dementia - Clinical Relevance, Methods of Assessment and Effects of TreatmentMelisa CastilloNessuna valutazione finora
- H.5.1 Antipsychotics PowerPoint 2016Documento55 pagineH.5.1 Antipsychotics PowerPoint 2016Ptrc Lbr LpNessuna valutazione finora
- Guidelines For The Management of Common Mental DisordersDocumento95 pagineGuidelines For The Management of Common Mental DisordersAruna HarikrishnanNessuna valutazione finora
- Neurocognitive Disorders by Hiwot G. (BSC, MSC)Documento113 pagineNeurocognitive Disorders by Hiwot G. (BSC, MSC)girmaw yidegNessuna valutazione finora
- Cap. Delirium - Bradley's Neurology in Clinical PracticDocumento11 pagineCap. Delirium - Bradley's Neurology in Clinical PracticArthur André RegovichiNessuna valutazione finora
- Dementia & DeliriumDocumento170 pagineDementia & Deliriummengaku0% (1)
- Bill of Materials and Estimates: ' ' Leona Bonghanoy YukoDocumento12 pagineBill of Materials and Estimates: ' ' Leona Bonghanoy YukoJupiter ZangelNessuna valutazione finora
- InstructionsDocumento1 paginaInstructionsJupiter ZangelNessuna valutazione finora
- Materials: TOTAL AMOUNT (Labor & Mat'ls) : 8,985.00Documento6 pagineMaterials: TOTAL AMOUNT (Labor & Mat'ls) : 8,985.00Jupiter ZangelNessuna valutazione finora
- KB Client Profile FormDocumento1 paginaKB Client Profile FormJupiter ZangelNessuna valutazione finora
- Construction MethodologyDocumento7 pagineConstruction MethodologyJupiter ZangelNessuna valutazione finora
- Verified HTT As of March 19, 2019Documento1 paginaVerified HTT As of March 19, 2019Jupiter ZangelNessuna valutazione finora
- Boq 17HF0066Documento5 pagineBoq 17HF0066Jupiter ZangelNessuna valutazione finora
- CLARIFIED NewPMOOffice - With VATDocumento57 pagineCLARIFIED NewPMOOffice - With VATJupiter ZangelNessuna valutazione finora
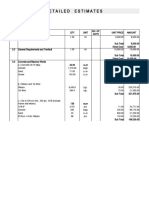
- Detailed EstimatesDocumento4 pagineDetailed Estimatesangelica ponceNessuna valutazione finora
- Envelope BDocumento3 pagineEnvelope BJupiter ZangelNessuna valutazione finora
- EquipmentDocumento1 paginaEquipmentJupiter ZangelNessuna valutazione finora
- Concrete and Reinforced ConcreteDocumento67 pagineConcrete and Reinforced ConcreteJupiter ZangelNessuna valutazione finora
- Bid Bulletin For 17HF0012Documento2 pagineBid Bulletin For 17HF0012Jupiter ZangelNessuna valutazione finora
- C o N S T R U C T I o N M e T H o D o L o G yDocumento4 pagineC o N S T R U C T I o N M e T H o D o L o G yJupiter Zangel100% (1)
- Pakigne, Minglanilla, Cebu Tel. No. (032) 516-5952, Telfax. No. (032) 490-4323 Cell. No. 09751854970 & 09424370235Documento4 paginePakigne, Minglanilla, Cebu Tel. No. (032) 516-5952, Telfax. No. (032) 490-4323 Cell. No. 09751854970 & 09424370235Jupiter ZangelNessuna valutazione finora
- AppDocumento3 pagineAppJupiter ZangelNessuna valutazione finora
- Bar Chart DrainageDocumento65 pagineBar Chart DrainageJupiter ZangelNessuna valutazione finora
- Civil Engineering Hydraulics - Essential Theory With Worked Examples 3rd EditionDocumento409 pagineCivil Engineering Hydraulics - Essential Theory With Worked Examples 3rd EditionCarlos AndresNessuna valutazione finora
- Presentation1 140907044532 Phpapp01Documento21 paginePresentation1 140907044532 Phpapp01Jupiter ZangelNessuna valutazione finora
- Beautiful Dancer': RomanizationDocumento8 pagineBeautiful Dancer': RomanizationJupiter ZangelNessuna valutazione finora
- 첫사랑의 기억Documento17 pagine첫사랑의 기억Jupiter ZangelNessuna valutazione finora
- DPWH - Cost EstimationDocumento63 pagineDPWH - Cost EstimationMarkSiapnodeVera89% (56)
- Bhel Ranipur Haridwar: Presented ByDocumento20 pagineBhel Ranipur Haridwar: Presented ByAnil ChauhanNessuna valutazione finora
- Footing Details 15cm Bothways 1:100m ScaleDocumento1 paginaFooting Details 15cm Bothways 1:100m ScaleJupiter ZangelNessuna valutazione finora
- Conflict With The Law PDFDocumento2 pagineConflict With The Law PDFJupiter ZangelNessuna valutazione finora
- 21 NewDocumento1 pagina21 NewJupiter ZangelNessuna valutazione finora
- Row ADocumento1 paginaRow AJupiter ZangelNessuna valutazione finora
- 11rooframing PlanDocumento1 pagina11rooframing PlanJupiter ZangelNessuna valutazione finora
- Brief-Depot-Bupe-Interim-Guidelines For South Australia Community Prescribers 2020 11 24Documento16 pagineBrief-Depot-Bupe-Interim-Guidelines For South Australia Community Prescribers 2020 11 24maco6708Nessuna valutazione finora
- Teaching Plan: General Santos Doctors' Medical School Foundation IncDocumento12 pagineTeaching Plan: General Santos Doctors' Medical School Foundation Incjay kusainNessuna valutazione finora
- Human Development Nursing QuestionsDocumento12 pagineHuman Development Nursing QuestionsMary SingletonNessuna valutazione finora
- Extracranial Carotid Artery Aneurysm - UpToDateDocumento25 pagineExtracranial Carotid Artery Aneurysm - UpToDateDiego RodriguesNessuna valutazione finora
- JWCE Catalog 2013Documento10 pagineJWCE Catalog 2013jsalas85Nessuna valutazione finora
- Una Coales 500 SBAsDocumento78 pagineUna Coales 500 SBAsAteeqNessuna valutazione finora
- Writing Effective Topic SentencesDocumento3 pagineWriting Effective Topic SentencesDerrith DunnNessuna valutazione finora
- Treating Addiction With TunesDocumento10 pagineTreating Addiction With TunesHajrudinNessuna valutazione finora
- CefepimeDocumento24 pagineCefepimedinniNessuna valutazione finora
- Occupational Therapy in Fatigue Management in MultDocumento8 pagineOccupational Therapy in Fatigue Management in MultghvntjbrbkNessuna valutazione finora
- Burning Mouth Syndrome GuideDocumento10 pagineBurning Mouth Syndrome GuiderosaNessuna valutazione finora
- Antwone FisherDocumento4 pagineAntwone FisherGalang PrakosoNessuna valutazione finora
- MBBS FINAL PROFESSIONAL MODEL QUESTIONS FOR ANNUAL 2009 MEDICINE (MCQSDocumento9 pagineMBBS FINAL PROFESSIONAL MODEL QUESTIONS FOR ANNUAL 2009 MEDICINE (MCQSemmaazizNessuna valutazione finora
- Chapter 1 Cognosy 1Documento4 pagineChapter 1 Cognosy 1vaibhavrathi100% (7)
- Acupuncture For TinnitusDocumento4 pagineAcupuncture For Tinnitussrimaauro5123Nessuna valutazione finora
- Study of Sickle Cell Anemia NewDocumento12 pagineStudy of Sickle Cell Anemia NewS.NagarajanNessuna valutazione finora
- Anesth ThesisDocumento11 pagineAnesth ThesisAkshay HariNessuna valutazione finora
- Tarsal Tunnel Syndrome - Physiopedia, Universal Access To Physiotherapy KnowledgeDocumento9 pagineTarsal Tunnel Syndrome - Physiopedia, Universal Access To Physiotherapy KnowledgeMuhammad Sahrul PatunruNessuna valutazione finora
- Comparative Analysis of Phenolic Contents and Total Antioxidant Capacity of Moringa Oleifera LamDocumento8 pagineComparative Analysis of Phenolic Contents and Total Antioxidant Capacity of Moringa Oleifera LamDessy Erlyani Mugita SariNessuna valutazione finora
- Bio-Electrode Therapy for Pain Relief and Addiction TreatmentDocumento19 pagineBio-Electrode Therapy for Pain Relief and Addiction TreatmentMokhtar Mohd100% (1)
- Distal Radius FractureDocumento16 pagineDistal Radius FractureDeneishMuruNessuna valutazione finora
- Infiltration Anaesthesia For Tympanoplasty: A Comparison of Dexmedetomidine and Clonidine As Adjuvants To Lignocaine and AdrenalineDocumento7 pagineInfiltration Anaesthesia For Tympanoplasty: A Comparison of Dexmedetomidine and Clonidine As Adjuvants To Lignocaine and AdrenalineIJAR JOURNALNessuna valutazione finora
- Bachelor of Physiotherpy: "A Case Study of Leprosy"Documento9 pagineBachelor of Physiotherpy: "A Case Study of Leprosy"NATIONAL XEROXNessuna valutazione finora
- Nursing Process Mcqs Session by Husain.ZDocumento14 pagineNursing Process Mcqs Session by Husain.ZInam ullah KhanNessuna valutazione finora
- Transgender Woman 'Raped 2,000 Times' in All-Male PrisonDocumento212 pagineTransgender Woman 'Raped 2,000 Times' in All-Male PrisonKrist YsabelleNessuna valutazione finora
- Fingertips Injury: Literature ReviewDocumento24 pagineFingertips Injury: Literature ReviewDonny Artya KesumaNessuna valutazione finora
- Bril (2002) - Validation of The Toronto Clinical Scoring System For Diabetic PolyneuropathyDocumento5 pagineBril (2002) - Validation of The Toronto Clinical Scoring System For Diabetic PolyneuropathyRicky WatariNessuna valutazione finora
- Volum Rezumate ZMN 2023 1Documento56 pagineVolum Rezumate ZMN 2023 1LuthienFreyNessuna valutazione finora
- Managing immune system disorders and immunosuppressant drugsDocumento2 pagineManaging immune system disorders and immunosuppressant drugsCorrine IvyNessuna valutazione finora
- Journal of Equine Veterinary Science: Original ResearchDocumento7 pagineJournal of Equine Veterinary Science: Original ResearchEduardo JaraNessuna valutazione finora