Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Nursing ProcessDocumento17 pagineThe Nursing ProcessElla Lobenaria100% (1)
- Physical ExaminationDocumento117 paginePhysical Examinationsasmita nayakNessuna valutazione finora
- Physical ExaminationgiDocumento61 paginePhysical ExaminationgiHei LeeNessuna valutazione finora
- Vomiting in PregnancyDocumento13 pagineVomiting in PregnancyPriyanka John100% (4)
- Clinical Examination of Companion AnimalsDocumento6 pagineClinical Examination of Companion AnimalsLouise Alysson OrtegaNessuna valutazione finora
- Health Assesment LectureDocumento15 pagineHealth Assesment LecturemeowzartNessuna valutazione finora
- Purina Body Condition Score DiagramDocumento1 paginaPurina Body Condition Score DiagramRonnel Anthony CelerioNessuna valutazione finora
- Askling ProtocolDocumento8 pagineAskling Protocolchrisschapendonk123Nessuna valutazione finora
- Nursing Care: Musculoskeletal SystemDocumento13 pagineNursing Care: Musculoskeletal SystemSukmawati PassiNessuna valutazione finora
- Assessment Mouth and Oropharynx LipsDocumento8 pagineAssessment Mouth and Oropharynx LipsQuinmarc LimNessuna valutazione finora
- (Undefined Series For Scimag) - Libgen - LiDocumento7 pagine(Undefined Series For Scimag) - Libgen - LiNicholas LimNessuna valutazione finora
- HEAS 1000 Health Assessment: Reflection of PracticeDocumento4 pagineHEAS 1000 Health Assessment: Reflection of PracticePreet ChahalNessuna valutazione finora
- Cerebral Palsy Amdekar SirDocumento42 pagineCerebral Palsy Amdekar SirVishalSapateNessuna valutazione finora
- Clinical Examination of Varicose VeinsDocumento6 pagineClinical Examination of Varicose VeinsR.m. AndriyanNessuna valutazione finora
- Chinese Herbology Study GuideDocumento58 pagineChinese Herbology Study Guidegiovanna2004100% (1)
- Health Assessment JarvisDocumento14 pagineHealth Assessment JarvisLilly Daye81% (31)
- CVS Study Guide 2023Documento28 pagineCVS Study Guide 2023Muhammad SulamanNessuna valutazione finora
- Assessment of The Abdomen ChecklistDocumento4 pagineAssessment of The Abdomen ChecklistKyle Randolf CuevasNessuna valutazione finora
- Po1 Po2 Po3 Po4 Po5 Po6 Po7 Po8 Po9 Po10 Po11 Po12 Po13 Po14Documento16 paginePo1 Po2 Po3 Po4 Po5 Po6 Po7 Po8 Po9 Po10 Po11 Po12 Po13 Po14Jerry AbleNessuna valutazione finora
- Abdominal Exam GuideDocumento5 pagineAbdominal Exam GuideNesma AdelNessuna valutazione finora
- Here are the zones in hand reflexology:Zone 1:Zone 2: Zone 3:Zone 4: Zone 5:Zone 6:Zone 7:Zone 8: Zone 9:Zone 10:Zone 11:Zone 12Documento12 pagineHere are the zones in hand reflexology:Zone 1:Zone 2: Zone 3:Zone 4: Zone 5:Zone 6:Zone 7:Zone 8: Zone 9:Zone 10:Zone 11:Zone 12Kim Caguioa100% (2)
- AssessmenDocumento1.083 pagineAssessmenluizamgoNessuna valutazione finora
- Breast Examination: 1. Iintroduction and Consent 2. ExposureDocumento4 pagineBreast Examination: 1. Iintroduction and Consent 2. ExposureNoor Ul AinNessuna valutazione finora
- Breast Exam GuideDocumento2 pagineBreast Exam GuideAyman HajeerNessuna valutazione finora
- Fundamentals of Nursing 9th Edition by Taylor Lynn Bartlett Test BankDocumento8 pagineFundamentals of Nursing 9th Edition by Taylor Lynn Bartlett Test Bankkathleenbaileytcgsrikobx100% (28)
- Case StudyDocumento6 pagineCase StudyEndla SriniNessuna valutazione finora
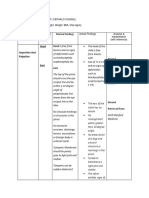
- Assessment Method Used Normal Findings: Head Head Is Free FromDocumento6 pagineAssessment Method Used Normal Findings: Head Head Is Free FromGil PerezNessuna valutazione finora
- Shamsurin CWU AwerzDocumento10 pagineShamsurin CWU AwerzAiman ArifinNessuna valutazione finora
- Examination of The BreastDocumento2 pagineExamination of The BreastAufi FillaNessuna valutazione finora