Potrebbero piacerti anche
- Diagnostics 12 00540Documento19 pagineDiagnostics 12 00540Arun Pratap SinghNessuna valutazione finora
- JAyurvedaCaseRep 2021 4 4 138 337115Documento9 pagineJAyurvedaCaseRep 2021 4 4 138 337115Aravind KumarNessuna valutazione finora
- Diagnosis and Management of Cerebral Small Vessel.9Documento18 pagineDiagnosis and Management of Cerebral Small Vessel.9Felipe MontorfanoNessuna valutazione finora
- Hong Et Al, 2022Documento7 pagineHong Et Al, 2022Bruno KudekenNessuna valutazione finora
- The Diagnosis and Management of Idiopathic Intracranial Hypertension and The Associated HeadacheDocumento10 pagineThe Diagnosis and Management of Idiopathic Intracranial Hypertension and The Associated HeadacheLatifatu ChoirunisaNessuna valutazione finora
- Q2 - 2017 - Uwaezuoke - The Role of Novel Biomarkers in Predicting DNDocumento11 pagineQ2 - 2017 - Uwaezuoke - The Role of Novel Biomarkers in Predicting DNbuat nugas28Nessuna valutazione finora
- Asymmetric Diabetic Retinopathy.18Documento9 pagineAsymmetric Diabetic Retinopathy.18Syeda F AmbreenNessuna valutazione finora
- Automated Detection of Vascular Abnormalities in Diabetic Retinopathy Using Morphological ThresholdingDocumento8 pagineAutomated Detection of Vascular Abnormalities in Diabetic Retinopathy Using Morphological ThresholdingpriyaNessuna valutazione finora
- Newsweek International - 28 05 2021Documento52 pagineNewsweek International - 28 05 2021Jose PirulliNessuna valutazione finora
- A Systematic Review and Meta-Analysis of Transcranial Direct-Current Stimulation Effects On Cognitive Function in Patients With Alzheimer 'S DiseaseDocumento10 pagineA Systematic Review and Meta-Analysis of Transcranial Direct-Current Stimulation Effects On Cognitive Function in Patients With Alzheimer 'S DiseaseAlireza MajdiNessuna valutazione finora
- Update On Normal Tension Glaucoma: Review ArticleDocumento10 pagineUpdate On Normal Tension Glaucoma: Review ArticleVlady BordaNessuna valutazione finora
- Paper 2 TTTTDocumento9 paginePaper 2 TTTTaislynpythonNessuna valutazione finora
- Endovascular Therapy For Cerebral Vein Thrombosis A Propensity-Matched Analysis of Anticoagulation in The Treatment of Cerebral Venous ThrombosisDocumento7 pagineEndovascular Therapy For Cerebral Vein Thrombosis A Propensity-Matched Analysis of Anticoagulation in The Treatment of Cerebral Venous Thrombosisguohong huNessuna valutazione finora
- Sensors: Detection of Diabetic Eye Disease From Retinal Images Using A Deep Learning Based Centernet ModelDocumento18 pagineSensors: Detection of Diabetic Eye Disease From Retinal Images Using A Deep Learning Based Centernet ModelSasha IraniNessuna valutazione finora
- Management of Acute StrokeDocumento12 pagineManagement of Acute StrokeAshok Vardhan Reddy TNessuna valutazione finora
- Ijo 69 525Documento10 pagineIjo 69 525Eduardo Espindola ElizaldeNessuna valutazione finora
- Small Vessel DiseaseDocumento21 pagineSmall Vessel Diseasepaola nabhanNessuna valutazione finora
- Admin, 014 - 979 - Franky Simarmata - GalleyDocumento6 pagineAdmin, 014 - 979 - Franky Simarmata - GalleyNoviani rosaNessuna valutazione finora
- Classification of Retinal Images For Diabetic Retinopathy at Non-Proliferative Stage Using ANFISDocumento7 pagineClassification of Retinal Images For Diabetic Retinopathy at Non-Proliferative Stage Using ANFISIIR indiaNessuna valutazione finora
- Intraoperative Desaturation During Thyroidectomy .27Documento2 pagineIntraoperative Desaturation During Thyroidectomy .27Annakay HudsonNessuna valutazione finora
- CohortDocumento8 pagineCohortShinichi KudoNessuna valutazione finora
- Knowledge-Based SystemsDocumento9 pagineKnowledge-Based SystemsAlmira CitraNessuna valutazione finora
- Mushtaq 2021 IOP Conf. Ser. Mater. Sci. Eng. 1070 012049Documento14 pagineMushtaq 2021 IOP Conf. Ser. Mater. Sci. Eng. 1070 0120493XTR3M3 ᜰ꙰ꦿ NJRNessuna valutazione finora
- Mtap S 23 08869Documento44 pagineMtap S 23 08869AkAnKsHa BaLiNessuna valutazione finora
- 016 - 1507 - Gede Bagus Mahendra Wirajaya - GalleyDocumento7 pagine016 - 1507 - Gede Bagus Mahendra Wirajaya - GalleynuraprianiNessuna valutazione finora
- Detection of Severity Level of Diabetic Retinopathy Using Bag of Features ModelDocumento8 pagineDetection of Severity Level of Diabetic Retinopathy Using Bag of Features ModelaaNessuna valutazione finora
- The Diagnostic and Clinical Approach To Pediatric Myocarditis: A Review of The Current LiteratureDocumento12 pagineThe Diagnostic and Clinical Approach To Pediatric Myocarditis: A Review of The Current LiteratureclaudyNessuna valutazione finora
- Base Pra Revisao TdcsDocumento7 pagineBase Pra Revisao TdcsHelena CysneirosNessuna valutazione finora
- Role of Red Cell Distribution Width in Severity Assessment of Ischemic StrokeDocumento5 pagineRole of Red Cell Distribution Width in Severity Assessment of Ischemic StrokeInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Systemic Approach On Immediate Evaluation and Management of Hyperacute StrokeDocumento25 pagineSystemic Approach On Immediate Evaluation and Management of Hyperacute StrokeDodik TugasworoNessuna valutazione finora
- Relationship Between Adult Subventricular Neurogenesis and Alzheimer's DiseaseDocumento9 pagineRelationship Between Adult Subventricular Neurogenesis and Alzheimer's DiseaseAlonso Sánchez DuránNessuna valutazione finora
- Detection and Classification of Arrhythmia Using An Explainable Deep Learning ModelDocumento9 pagineDetection and Classification of Arrhythmia Using An Explainable Deep Learning ModelComisión Académica FCM - UNAHNessuna valutazione finora
- Diabetic Retinopathy Detection and Classification Using Hybrid Multiclass SVM Classifier and Deeplearning TechniquesDocumento13 pagineDiabetic Retinopathy Detection and Classification Using Hybrid Multiclass SVM Classifier and Deeplearning TechniquesVishnu Vardhan CreationsNessuna valutazione finora
- Role of CT and MRI in Stroke DiagnosisDocumento51 pagineRole of CT and MRI in Stroke DiagnosisBokuma KuciNessuna valutazione finora
- Strechmark ReviewDocumento13 pagineStrechmark Review郭先薈Nessuna valutazione finora
- Sonography of Abdomen and PelvisDocumento2 pagineSonography of Abdomen and PelvisAbhishek RankaNessuna valutazione finora
- JNeurosciRuralPract 2013 4 4 461 120212Documento5 pagineJNeurosciRuralPract 2013 4 4 461 120212andrada67Nessuna valutazione finora
- MigrainDocumento19 pagineMigrainSecondhand XoxoNessuna valutazione finora
- Fneur 13 836997Documento8 pagineFneur 13 836997damaryandreaNessuna valutazione finora
- Retinal ImagesDocumento7 pagineRetinal ImagesKallur AkshathaNessuna valutazione finora
- Zapping The Brain and Nerves Could Treat Long COVID - IEEE SpectrumDocumento1 paginaZapping The Brain and Nerves Could Treat Long COVID - IEEE Spectrumtd5xb7w4dpNessuna valutazione finora
- Vision Research: Stephanie K. Lynch, Michael D. AbràmoffDocumento7 pagineVision Research: Stephanie K. Lynch, Michael D. Abràmoffanka_mihaelaNessuna valutazione finora
- Predominance of Cellular Edema in Traumatic Brain Swelling in Patients With Severe Head InjuriesDocumento11 paginePredominance of Cellular Edema in Traumatic Brain Swelling in Patients With Severe Head InjuriesRiyaldi Dwipa AnugrahNessuna valutazione finora
- Jurnal ODDocumento7 pagineJurnal ODDhimas Arief DharmawanNessuna valutazione finora
- Nejmicm 1214985Documento1 paginaNejmicm 1214985Lucas AnicichNessuna valutazione finora
- Ayurvedic Management of Prurigo Nodularis at Scalp - A Case ReportDocumento5 pagineAyurvedic Management of Prurigo Nodularis at Scalp - A Case ReportmskchoudhuriNessuna valutazione finora
- Long Term Outcome of Coronary Artery Dilatation in Kawasaki DiseaseDocumento5 pagineLong Term Outcome of Coronary Artery Dilatation in Kawasaki DiseaseRahma Ira MustikasariNessuna valutazione finora
- Definiendio Enfermedad Renal Aguda 2021 NephronDocumento4 pagineDefiniendio Enfermedad Renal Aguda 2021 NephronGabino Alexander Liviac CrisostomoNessuna valutazione finora
- Cerebral Small Vessel Disease and Vascular.15Documento12 pagineCerebral Small Vessel Disease and Vascular.15Олег ЛевинNessuna valutazione finora
- Update On Normal Tension Glaucoma: Review ArticleDocumento5 pagineUpdate On Normal Tension Glaucoma: Review ArticleNur Rakhma AkmaliaNessuna valutazione finora
- A Review On Ayurvedic Approach To Age Related Changes in NetraDocumento3 pagineA Review On Ayurvedic Approach To Age Related Changes in NetraEditor IJTSRD0% (1)
- Stroke Compendium: Vascular Cognitive ImpairmentDocumento20 pagineStroke Compendium: Vascular Cognitive ImpairmentJuan Jose Eraso OsorioNessuna valutazione finora
- 1 s2.0 S2352873719300770 MainDocumento17 pagine1 s2.0 S2352873719300770 Mainstevenburrow06Nessuna valutazione finora
- Jaha 121 025205Documento32 pagineJaha 121 025205julinka beyla yansonNessuna valutazione finora
- Jurnal Neuralgia TrigerminalDocumento13 pagineJurnal Neuralgia TrigerminallarasatiNessuna valutazione finora
- DENGUE FEVER Test Report Format Example Sample Template Drlogy Lab ReportDocumento1 paginaDENGUE FEVER Test Report Format Example Sample Template Drlogy Lab ReportBhojraj SinghNessuna valutazione finora
- Circadian Patterns of ST Elevation Myocardial Infarction in The New MillenniumDocumento7 pagineCircadian Patterns of ST Elevation Myocardial Infarction in The New MillenniumYanna RizkiaNessuna valutazione finora
- 10 1001@jama 2017 0059Documento2 pagine10 1001@jama 2017 0059Fernando GeldresNessuna valutazione finora
- WHO HTM TB 2016.06 EngDocumento16 pagineWHO HTM TB 2016.06 EngTammy Utami DewiNessuna valutazione finora
- Tuberculosis Surveillance Monitoring Europe 2018 Rev1 PDFDocumento206 pagineTuberculosis Surveillance Monitoring Europe 2018 Rev1 PDFYanna RizkiaNessuna valutazione finora
- HTN PamphletDocumento20 pagineHTN PamphletMaria Ivy MendozaNessuna valutazione finora
- Nutritional Therapy in Major BurnsDocumento6 pagineNutritional Therapy in Major BurnsRuth Danielle GasconNessuna valutazione finora
- vhrm0204 371Documento8 paginevhrm0204 371Yanna RizkiaNessuna valutazione finora
- HTN PamphletDocumento20 pagineHTN PamphletMaria Ivy MendozaNessuna valutazione finora
- sr11 252Documento48 paginesr11 252arulrajiv1Nessuna valutazione finora
- APA - DSM5 - Level 2 Anxiety Adult PDFDocumento3 pagineAPA - DSM5 - Level 2 Anxiety Adult PDFDiana TodeaNessuna valutazione finora
- JNC 8Documento14 pagineJNC 8amiwahyuniNessuna valutazione finora
- Contemporary Diagnosis and Management of Preterm LaborDocumento4 pagineContemporary Diagnosis and Management of Preterm LaborYanna RizkiaNessuna valutazione finora
- Hiv WhoDocumento480 pagineHiv Whoأبو أويس شرف الدينNessuna valutazione finora
- Srep 45870Documento11 pagineSrep 45870Yanna RizkiaNessuna valutazione finora
- 149 Ipp Jan March 2017 9Documento9 pagine149 Ipp Jan March 2017 9Yanna RizkiaNessuna valutazione finora
- Routine Newborn Assessment PDFDocumento17 pagineRoutine Newborn Assessment PDFYanna RizkiaNessuna valutazione finora
- Annular Lesions in Dermatology PDFDocumento6 pagineAnnular Lesions in Dermatology PDFYanna RizkiaNessuna valutazione finora
- BMJ c4416 FullDocumento8 pagineBMJ c4416 FullLukman Al-HafizNessuna valutazione finora
- Tyg AcylDocumento30 pagineTyg AcylYanna RizkiaNessuna valutazione finora
- Anes CH 32Documento12 pagineAnes CH 32Yanna RizkiaNessuna valutazione finora
- Sepsis Pathophysiology and Clinical ManagementDocumento20 pagineSepsis Pathophysiology and Clinical Managementkartini ciatawiNessuna valutazione finora
- ACC16 ProgramPDF PATH AcuteCoronaryDocumento23 pagineACC16 ProgramPDF PATH AcuteCoronaryIsrael de la CruzNessuna valutazione finora
- Biomarkers For Pediatrics Sepsis and Pediatric ShockDocumento15 pagineBiomarkers For Pediatrics Sepsis and Pediatric ShockYanna RizkiaNessuna valutazione finora
- Overview SepsisDocumento13 pagineOverview SepsisYanna RizkiaNessuna valutazione finora
- Management of Criticalli Ill Child SepsisDocumento4 pagineManagement of Criticalli Ill Child SepsisYanna RizkiaNessuna valutazione finora
- EGDT in Pediatric Septic ShockDocumento11 pagineEGDT in Pediatric Septic ShockYanna RizkiaNessuna valutazione finora
- Differences Between Adult and Pediatric Septic ShockDocumento7 pagineDifferences Between Adult and Pediatric Septic ShockYanna RizkiaNessuna valutazione finora
- Important Considerations For Diagnosing and Managing Sever Pediatric SepsisDocumento12 pagineImportant Considerations For Diagnosing and Managing Sever Pediatric SepsisYanna RizkiaNessuna valutazione finora
- Procalcitnonin and CRP in SIRS and SepsisDocumento9 pagineProcalcitnonin and CRP in SIRS and SepsisYanna RizkiaNessuna valutazione finora
- NO. TGL Nama RM: JANUARI 2014Documento481 pagineNO. TGL Nama RM: JANUARI 2014DewieqJunexNessuna valutazione finora
- Bergey S ManualDocumento1.130 pagineBergey S Manualanalista LMH2Nessuna valutazione finora
- Pneumonia Si Pleurezia Parapneumonica: Agentii Etiologici Cei Mai FrecventiDocumento2 paginePneumonia Si Pleurezia Parapneumonica: Agentii Etiologici Cei Mai FrecventiCatalina Andreea CucutaNessuna valutazione finora
- About Monkey PoxDocumento3 pagineAbout Monkey PoxObakoma Josiah100% (1)
- Oswego E 2012 PDFDocumento14 pagineOswego E 2012 PDFA SeulNessuna valutazione finora
- Health Declaration Form Health Declaration FormDocumento1 paginaHealth Declaration Form Health Declaration FormGerone NavaeraNessuna valutazione finora
- Streptococcus Pneumoniae Staphylococci Faculty: Dr. Alvin FoxDocumento32 pagineStreptococcus Pneumoniae Staphylococci Faculty: Dr. Alvin Foxdanish sultan100% (1)
- How To Prevent PhlebitisDocumento8 pagineHow To Prevent PhlebitisAffrida Nurlily Chintya WidariNessuna valutazione finora
- Culture MediaDocumento4 pagineCulture MediaHabibur RahamanNessuna valutazione finora
- A Brief History of Vaccines and Vaccination.Documento20 pagineA Brief History of Vaccines and Vaccination.sameer100% (2)
- Additional Material. Microbiology - Class 6.Documento3 pagineAdditional Material. Microbiology - Class 6.Rajveer KaurNessuna valutazione finora
- Questions ExplanationDocumento63 pagineQuestions ExplanationnomintmNessuna valutazione finora
- Lesson PlanDocumento14 pagineLesson PlanAnkit KotnalaNessuna valutazione finora
- FCM Group3 FilariasisDocumento90 pagineFCM Group3 FilariasisAngela CaguitlaNessuna valutazione finora
- Typhoid Fever PathophysiologyDocumento1 paginaTyphoid Fever Pathophysiologynesjyn75% (4)
- MicrobiologyDocumento52 pagineMicrobiologyhema100% (1)
- Infectious Disease Questions 1Documento36 pagineInfectious Disease Questions 1Jelly BeansNessuna valutazione finora
- BIOL 3162 Lab 2-Introduction To Microbial Biotech Techniques ADocumento7 pagineBIOL 3162 Lab 2-Introduction To Microbial Biotech Techniques Arube10000Nessuna valutazione finora
- What Is A Urinary Tract InfectionDocumento3 pagineWhat Is A Urinary Tract InfectionVanessa MendezNessuna valutazione finora
- Nacker - 2011 - The-Impact-Of-Climate-Change-And-Other-Factors-On-Zoonotic-DiseasesDocumento6 pagineNacker - 2011 - The-Impact-Of-Climate-Change-And-Other-Factors-On-Zoonotic-Diseasesrodrigocamiloo97Nessuna valutazione finora
- COURSE Syllabus: The University of Jordan Accreditation & Quality Assurance CenterDocumento10 pagineCOURSE Syllabus: The University of Jordan Accreditation & Quality Assurance CenterlanaNessuna valutazione finora
- Aerobic Gram Positive BacilliDocumento36 pagineAerobic Gram Positive BacilliMac Kevin MandapNessuna valutazione finora
- AIDS/HIV An Overview 1Documento7 pagineAIDS/HIV An Overview 1tiffrenfitNessuna valutazione finora
- Eskape PathogensDocumento8 pagineEskape PathogensMarina DomencoNessuna valutazione finora
- Group 3: Widia Yuni Pratiwi Sari Saiba Ningrum Ni Putu Rika Fadlunnisa Tiya MutiaraDocumento12 pagineGroup 3: Widia Yuni Pratiwi Sari Saiba Ningrum Ni Putu Rika Fadlunnisa Tiya MutiaraWidia YuniNessuna valutazione finora
- Dengue DOHDocumento16 pagineDengue DOHGehlatin Tumanan100% (1)
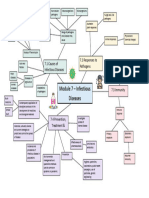
- Module 7 Mind Map BiologyDocumento1 paginaModule 7 Mind Map BiologyAltSpace TimeNessuna valutazione finora
- LAB 3 - Microscopy, Gram Staining, Coproparasitol 2022-2023Documento5 pagineLAB 3 - Microscopy, Gram Staining, Coproparasitol 2022-2023Silvia UngureanuNessuna valutazione finora
- Final Results Report: Curative Labs Inc. 3330 New York Ave NE Washington, DC 20002Documento1 paginaFinal Results Report: Curative Labs Inc. 3330 New York Ave NE Washington, DC 20002Aidan NicholsNessuna valutazione finora
- Patho DHFDocumento2 paginePatho DHFPhillip GoNessuna valutazione finora