Potrebbero piacerti anche
- Diabetes Fix PDFDocumento162 pagineDiabetes Fix PDFRicardo Bernal100% (3)
- Microbiologist: 3.1.5 Isolation & Gram StainingDocumento5 pagineMicrobiologist: 3.1.5 Isolation & Gram Stainingapi-534896073Nessuna valutazione finora
- Surgery Okell Notes 2Documento205 pagineSurgery Okell Notes 2Youzuf Iqbal100% (1)
- KPI-Surgery VolumeDocumento1 paginaKPI-Surgery Volumeangeli punoNessuna valutazione finora
- Approach 4 Standard Precautions Icon PDF 672KBDocumento1 paginaApproach 4 Standard Precautions Icon PDF 672KBElaine MacalandaNessuna valutazione finora
- MS ByLaws 2018Documento53 pagineMS ByLaws 2018محمد عقيليNessuna valutazione finora
- Cordis Case Study PDFDocumento29 pagineCordis Case Study PDFsingh242Nessuna valutazione finora
- Acute Bronchitis - FinalDocumento28 pagineAcute Bronchitis - FinalJied100% (6)
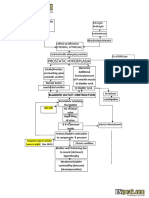
- Benign Prostatic Hyperplasia - BPH - Pathophysiology - Schematic DiagramDocumento2 pagineBenign Prostatic Hyperplasia - BPH - Pathophysiology - Schematic DiagramSimran JosanNessuna valutazione finora
- JCI International Library of Measures ANIK BUKUDocumento325 pagineJCI International Library of Measures ANIK BUKUnurulNessuna valutazione finora
- Seminar JCI - 9 Feb 2012Documento16 pagineSeminar JCI - 9 Feb 2012Mahardika PertiwiNessuna valutazione finora
- Handout Core CompetenciesDocumento4 pagineHandout Core CompetenciesAi CaNessuna valutazione finora
- JCI Update 2011Documento26 pagineJCI Update 2011Bayuaji SismantoNessuna valutazione finora
- Hospital Service Quality AsDocumento20 pagineHospital Service Quality AsNurulfitrahhafidNessuna valutazione finora
- OPPE Dokter Di RS - EnglishDocumento70 pagineOPPE Dokter Di RS - EnglishKetut Widiyasa BonaNessuna valutazione finora
- Risk Assessment For Pressure InjuryDocumento34 pagineRisk Assessment For Pressure InjuryNandarNessuna valutazione finora
- Mod2 - Ch3 - Health IndicatorsDocumento13 pagineMod2 - Ch3 - Health IndicatorsSara Sunabara100% (1)
- Daftar Panduan JCIDocumento12 pagineDaftar Panduan JCIEko Wahyu AgustinNessuna valutazione finora
- Infection Prevention and Control Assessment Tool For Outpatient SettingsDocumento22 pagineInfection Prevention and Control Assessment Tool For Outpatient SettingsVera IndrawatiNessuna valutazione finora
- MSF OCA NCD Guidelines v4 2018Documento138 pagineMSF OCA NCD Guidelines v4 2018Imad Q. KhaleelNessuna valutazione finora
- Who Patient SafetyDocumento14 pagineWho Patient SafetyJuwita Valen RamadhanniaNessuna valutazione finora
- Name of PolicyDocumento11 pagineName of PolicysuryaniNessuna valutazione finora
- Hospital Committees Part4Documento7 pagineHospital Committees Part4fatmanajehNessuna valutazione finora
- Emergency Nurses Association (ENA)Documento5 pagineEmergency Nurses Association (ENA)Ngu W PhooNessuna valutazione finora
- Assessment and Re-Assessment of Patients According To The Scope of ServiceDocumento9 pagineAssessment and Re-Assessment of Patients According To The Scope of Servicegiya nursingNessuna valutazione finora
- 05 Figure2 1 Environmental Tour FormDocumento8 pagine05 Figure2 1 Environmental Tour FormErna WahyuningtyasNessuna valutazione finora
- Hakim Seikh CaseDocumento14 pagineHakim Seikh Caseronn13nNessuna valutazione finora
- Sentinel Events: Vidya PrasadDocumento21 pagineSentinel Events: Vidya PrasadTOUSHIFAHEMEDNessuna valutazione finora
- Scripps Hospital Patient Visitor Policy PDFDocumento2 pagineScripps Hospital Patient Visitor Policy PDFcode4saleNessuna valutazione finora
- NEWS2 Final Report - 0 PDFDocumento77 pagineNEWS2 Final Report - 0 PDFIvoria Septiani GuloNessuna valutazione finora
- JCI International Library of MeasuresDocumento261 pagineJCI International Library of MeasuresDedy Haris DeswandarNessuna valutazione finora
- Strategies To Improve Handoff CommunicationDocumento2 pagineStrategies To Improve Handoff CommunicationJames SimmonsNessuna valutazione finora
- CHA Hospital Activation of The Emergency Operations Plan ChecklistDocumento5 pagineCHA Hospital Activation of The Emergency Operations Plan Checklistraysub159Nessuna valutazione finora
- A P Policy & Procedure: Ntibiotic OlicyDocumento24 pagineA P Policy & Procedure: Ntibiotic Olicyvijay kumarNessuna valutazione finora
- Executive Summary On Bio-Medical Waste Management: Quantitative Techniques and Research Methods in Management AssignmentDocumento5 pagineExecutive Summary On Bio-Medical Waste Management: Quantitative Techniques and Research Methods in Management AssignmentMayuri VarkeyNessuna valutazione finora
- Define Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalDocumento15 pagineDefine Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalAbdul RahamanNessuna valutazione finora
- Infection Control Program Flow ChartDocumento1 paginaInfection Control Program Flow ChartAnonymous ORleRrNessuna valutazione finora
- Self Assessment ToolkitDocumento54 pagineSelf Assessment ToolkitshekarNessuna valutazione finora
- Flow Chart For Adult Cardio-Pulmonary Resuscitation (Adult CPR)Documento1 paginaFlow Chart For Adult Cardio-Pulmonary Resuscitation (Adult CPR)Lia IshakNessuna valutazione finora
- Medication Policy Sept 13Documento3 pagineMedication Policy Sept 13parkadminNessuna valutazione finora
- On WHO Standards and RecommendationsDocumento62 pagineOn WHO Standards and Recommendationspoonam@ims0% (1)
- IPSG PresentationDocumento38 pagineIPSG Presentationmuhammed shamaa100% (1)
- Quality Introduction: Performance IndicatorDocumento28 pagineQuality Introduction: Performance IndicatorLiza VarouqaNessuna valutazione finora
- Patient Safety: What Should We Be Trying To Communicate?Documento32 paginePatient Safety: What Should We Be Trying To Communicate?cicaklomenNessuna valutazione finora
- Final Rwanda Hospital Accreditation Standards Performance Assessment 3 Edition 2022Documento168 pagineFinal Rwanda Hospital Accreditation Standards Performance Assessment 3 Edition 2022john peter BamporikiNessuna valutazione finora
- Safety Grades ExplanationDocumento2 pagineSafety Grades ExplanationWXYZ-TV Channel 7 DetroitNessuna valutazione finora
- Annual Plan: Infection Prevention & Control DepartmentDocumento3 pagineAnnual Plan: Infection Prevention & Control DepartmentSherina Edding0% (1)
- Oncology Scope of ServicesDocumento2 pagineOncology Scope of ServicesJaisurya SharmaNessuna valutazione finora
- Code Purple Procedure PDFDocumento5 pagineCode Purple Procedure PDFdidikNessuna valutazione finora
- 1.medication ErrorsDocumento25 pagine1.medication ErrorshussainNessuna valutazione finora
- JCI QUESTIONNAIRE-PCI Dept.Documento6 pagineJCI QUESTIONNAIRE-PCI Dept.Rabiya Sajjad100% (2)
- Principles of Oncology and Outline of ManagementDocumento78 paginePrinciples of Oncology and Outline of ManagementPavan JonnadaNessuna valutazione finora
- A Proven Pathway To AccreditationDocumento25 pagineA Proven Pathway To AccreditationkukunNessuna valutazione finora
- Patient Satisfaction 1Documento37 paginePatient Satisfaction 1Bidyut RayNessuna valutazione finora
- Hospital ETP STP Paper PDFDocumento7 pagineHospital ETP STP Paper PDFamitkenNessuna valutazione finora
- Obeid Specialized Hospital - Riyadh: Key Performance Indiactors Second Quarter - 2019Documento29 pagineObeid Specialized Hospital - Riyadh: Key Performance Indiactors Second Quarter - 2019LovelydePerioNessuna valutazione finora
- Quality and HospitalDocumento6 pagineQuality and HospitalKuldeep BajajNessuna valutazione finora
- Safety ChecklistDocumento8 pagineSafety ChecklistdharmaNessuna valutazione finora
- 2007 International Patient Safety GoalsDocumento1 pagina2007 International Patient Safety GoalsElias Baraket FreijyNessuna valutazione finora
- TED-FRM-002E (2) - Training Needs Assessment ChecklistDocumento2 pagineTED-FRM-002E (2) - Training Needs Assessment ChecklistAmira SantiagoNessuna valutazione finora
- Patient Safety Organization A Complete Guide - 2020 EditionDa EverandPatient Safety Organization A Complete Guide - 2020 EditionNessuna valutazione finora
- Healthcare Environmental Services A Complete Guide - 2020 EditionDa EverandHealthcare Environmental Services A Complete Guide - 2020 EditionNessuna valutazione finora
- 1.overview of JCI 2017Documento18 pagine1.overview of JCI 2017Nesti AgustNessuna valutazione finora
- SpecialistDocumento1 paginaSpecialistShashiNessuna valutazione finora
- Facts Speak Louder Than The Silent Scream 03-02Documento6 pagineFacts Speak Louder Than The Silent Scream 03-02ProgressTXNessuna valutazione finora
- Broad Spectrum AntibioticsDocumento17 pagineBroad Spectrum AntibioticsRabi ShahNessuna valutazione finora
- Treatment of Bipolar DisorderDocumento20 pagineTreatment of Bipolar DisorderShana Wl100% (1)
- Chiropractic and Physical Therapies (PDFDrive)Documento279 pagineChiropractic and Physical Therapies (PDFDrive)Pierre NotserNessuna valutazione finora
- Multiple SclerosisDocumento5 pagineMultiple SclerosisEliDavidNessuna valutazione finora
- Running Head: Critical Reflection 1Documento5 pagineRunning Head: Critical Reflection 1api-313097878Nessuna valutazione finora
- Nursing Process OUTPUTDocumento5 pagineNursing Process OUTPUTfima_njNessuna valutazione finora
- Hiatus Hernia - Chinese Herbs, Chinese Medicine, AcupunctureDocumento6 pagineHiatus Hernia - Chinese Herbs, Chinese Medicine, AcupunctureCarlCordNessuna valutazione finora
- Specimen Referral Networks FinalDocumento132 pagineSpecimen Referral Networks FinalMigori ArtNessuna valutazione finora
- Ectopic Pregnancy (m104)Documento13 pagineEctopic Pregnancy (m104)Alphine DalgoNessuna valutazione finora
- 0003IADDocumento12 pagine0003IADRika AzyenelaNessuna valutazione finora
- Name: Prado, Catherine A. Year and Section: BSN III-B Module 4 ReflectionDocumento2 pagineName: Prado, Catherine A. Year and Section: BSN III-B Module 4 ReflectionCatherine PradoNessuna valutazione finora
- Putney Rehab Centre TimetableDocumento2 paginePutney Rehab Centre Timetableapi-280584977Nessuna valutazione finora
- Sheehan's Syndrome PathophysiologyDocumento2 pagineSheehan's Syndrome PathophysiologyirismgallNessuna valutazione finora
- Bacteria and Immune Defenses: Helicobacter PyloriDocumento4 pagineBacteria and Immune Defenses: Helicobacter PyloriMary Rose SJ JimenezNessuna valutazione finora
- Recognizing A Technically Adequate Chest X-RayDocumento30 pagineRecognizing A Technically Adequate Chest X-RayagungNessuna valutazione finora
- Research Critiques and PICOT QuestionDocumento10 pagineResearch Critiques and PICOT QuestionSamwel KangyNessuna valutazione finora
- 【Invitation】Educational Webinar Series for Asia-Pacific Pediatrics EP physicians and early career EPsDocumento7 pagine【Invitation】Educational Webinar Series for Asia-Pacific Pediatrics EP physicians and early career EPsSantoso 9JimmyNessuna valutazione finora
- G6PD Brochure 2017Documento3 pagineG6PD Brochure 2017Je Ann Catherine FeliasNessuna valutazione finora
- International Journal of Pediatric Research Ijpr 9 113Documento4 pagineInternational Journal of Pediatric Research Ijpr 9 113VsbshNessuna valutazione finora
- Egypt Cochlear PresentationDocumento30 pagineEgypt Cochlear PresentationAhmad Salahuddien100% (1)
- Anatomy of The Genitourinary TractDocumento5 pagineAnatomy of The Genitourinary TractQonitaaNessuna valutazione finora
- College of Nursing: Cebu Normal UniversityDocumento3 pagineCollege of Nursing: Cebu Normal UniversityShiva TorinsNessuna valutazione finora
- MK SurgeryDocumento900 pagineMK Surgerybovarep216Nessuna valutazione finora