Potrebbero piacerti anche
- Ward Census OB Ward Aug 26 DUTYDocumento26 pagineWard Census OB Ward Aug 26 DUTYRobz Apacionado100% (1)
- Conversion From Mmol, Arthritis DifferentiationDocumento7 pagineConversion From Mmol, Arthritis DifferentiationRobz ApacionadoNessuna valutazione finora
- Blank RXDocumento2 pagineBlank RXRobz ApacionadoNessuna valutazione finora
- Blank RXDocumento2 pagineBlank RXRobz ApacionadoNessuna valutazione finora
- Diagnostic Examinations 1. Physical Examination: B. Plain X-Ray FilmDocumento1 paginaDiagnostic Examinations 1. Physical Examination: B. Plain X-Ray FilmRobz ApacionadoNessuna valutazione finora
- Malaria Control ProgramDocumento144 pagineMalaria Control ProgramRobz ApacionadoNessuna valutazione finora
- GuidelinesDocumento2 pagineGuidelinesRobz ApacionadoNessuna valutazione finora
- Eat Heart SmartDocumento6 pagineEat Heart SmartitseminaryNessuna valutazione finora
- Yfc Songs 2Documento5 pagineYfc Songs 2Robz ApacionadoNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- OTM Rate Offering TypeDocumento5 pagineOTM Rate Offering Typevamc232855Nessuna valutazione finora
- Attachment 5 Transmission Line Design Criteria - AshxDocumento33 pagineAttachment 5 Transmission Line Design Criteria - AshxAnonymous ep7LE5ZdP5Nessuna valutazione finora
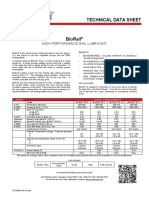
- Technical Data Sheet: High Performance Rail LubricantDocumento1 paginaTechnical Data Sheet: High Performance Rail LubricantvarunchNessuna valutazione finora
- History of Waterlooville, John RegerDocumento56 pagineHistory of Waterlooville, John RegerAnonymous UgVOzaNessuna valutazione finora
- HOMOGENIZATION OF BULK MATERIAL IN Chevron PileDocumento7 pagineHOMOGENIZATION OF BULK MATERIAL IN Chevron Pilesupendra phuyal100% (1)
- Party Area of TourDocumento122 pagineParty Area of Tourapi-3707678100% (1)
- Reporting - Analysis - Equipment - Failures PDFDocumento18 pagineReporting - Analysis - Equipment - Failures PDFPushpender Kumar Singh100% (1)
- NDLS KopDocumento2 pagineNDLS KopJatin DhawanNessuna valutazione finora
- Full ResearchDocumento14 pagineFull ResearchKassandra Peralta MadarangNessuna valutazione finora
- Handbook Foundation Form Work Rebar ConcreteDocumento216 pagineHandbook Foundation Form Work Rebar ConcretebittuchintuNessuna valutazione finora
- Coogee International Development Inc.: 2 Flr. Optima Bldg. 221 Salcedo ST., Cor. Gamboa ST., Legaspi Village, Makati CityDocumento34 pagineCoogee International Development Inc.: 2 Flr. Optima Bldg. 221 Salcedo ST., Cor. Gamboa ST., Legaspi Village, Makati CityCyril BayugaNessuna valutazione finora
- CBTC (Communication Based Train Control) : System and DevelopmentDocumento8 pagineCBTC (Communication Based Train Control) : System and DevelopmentsankardevNessuna valutazione finora
- The LAND PUBLIC TRANSPORT ACT 2010 Improving Malaysian Traffic ConditionsDocumento3 pagineThe LAND PUBLIC TRANSPORT ACT 2010 Improving Malaysian Traffic ConditionsTengku Muhammad SyukranNessuna valutazione finora
- Bridge Maintenance On Indian RailwaysDocumento23 pagineBridge Maintenance On Indian Railwaysvbs_rly4375Nessuna valutazione finora
- Flyoverbridge 1Documento23 pagineFlyoverbridge 1Sheikh UbaidNessuna valutazione finora
- Site Suitability Report S33HF and C04XJ: Vacant Land and Thames Water Hammersmith Pumping Station, Chancellors RoadDocumento75 pagineSite Suitability Report S33HF and C04XJ: Vacant Land and Thames Water Hammersmith Pumping Station, Chancellors Roadinfo1639Nessuna valutazione finora
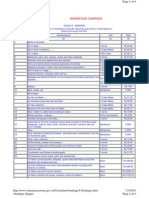
- Wharfage ChargesDocumento4 pagineWharfage ChargessyedalimechNessuna valutazione finora
- Jumbled SentenceDocumento8 pagineJumbled SentenceSAKTHI SAKTHINessuna valutazione finora
- L.N. 211 of 1974: Cap 59J - Factories and Industrial Undertakings (Lifting Appliances and Lifting Gear) RegulationsDocumento13 pagineL.N. 211 of 1974: Cap 59J - Factories and Industrial Undertakings (Lifting Appliances and Lifting Gear) RegulationsLAMNessuna valutazione finora
- Smartron: Focused To The MaxDocumento8 pagineSmartron: Focused To The Maxcosty_transNessuna valutazione finora
- One Year After Hokuriku Shinkansen OpeningDocumento8 pagineOne Year After Hokuriku Shinkansen OpeningMay RatchaNessuna valutazione finora
- Ee660 2017 Spring Materials Week 04 SlidesDocumento40 pagineEe660 2017 Spring Materials Week 04 SlidesqaeszNessuna valutazione finora
- SCOMI-Page 24 To ProxyForm (2.3MB)Documento175 pagineSCOMI-Page 24 To ProxyForm (2.3MB)Athira HusnaNessuna valutazione finora
- SST PPT CH 3Documento11 pagineSST PPT CH 3Sana AnsariNessuna valutazione finora
- Dynamic Prestress HDPE Pipe Brochure PDFDocumento4 pagineDynamic Prestress HDPE Pipe Brochure PDFdhopat kalpeshNessuna valutazione finora
- Urban Streets: Lecture Notes in Transportation Systems EngineeringDocumento21 pagineUrban Streets: Lecture Notes in Transportation Systems EngineeringHanafiahHamzahNessuna valutazione finora
- Hollywood Bohemia: The Roots of Progressive Politics in Rob Wagner's ScriptDocumento254 pagineHollywood Bohemia: The Roots of Progressive Politics in Rob Wagner's ScriptRob Leicester WagnerNessuna valutazione finora
- RailSingleTrackCANT SeccionTipo InglesDocumento9 pagineRailSingleTrackCANT SeccionTipo InglesCarlos Roberto Ugalde ArellanoNessuna valutazione finora
- GPT Is Sleeper SupplierDocumento22 pagineGPT Is Sleeper SupplieratulNessuna valutazione finora
- Texa Motor Truck 39.0.0 Latest Version Application List en-GBDocumento180 pagineTexa Motor Truck 39.0.0 Latest Version Application List en-GBkallatisNessuna valutazione finora