Potrebbero piacerti anche
- The Prevalence and Risk FactorsDocumento17 pagineThe Prevalence and Risk FactorsLilia ScutelnicNessuna valutazione finora
- ActivityStability of Human PepsinDocumento4 pagineActivityStability of Human PepsinLilia ScutelnicNessuna valutazione finora
- Association of Laryngopharyngeal PDFDocumento8 pagineAssociation of Laryngopharyngeal PDFLilia ScutelnicNessuna valutazione finora
- Videostroboscopy in Laryngopharengeal RefluxDocumento5 pagineVideostroboscopy in Laryngopharengeal RefluxLilia ScutelnicNessuna valutazione finora
- The Prevalence of Laryngeal PathologyDocumento7 pagineThe Prevalence of Laryngeal PathologyLilia ScutelnicNessuna valutazione finora
- English Today Vol.1 Varianta 2 PDFDocumento93 pagineEnglish Today Vol.1 Varianta 2 PDFDan CelacNessuna valutazione finora
- 0003489414532777Documento10 pagine0003489414532777Lilia ScutelnicNessuna valutazione finora
- 0 GERD Abstractbook 11FINAL 67833Documento174 pagine0 GERD Abstractbook 11FINAL 67833Lilia ScutelnicNessuna valutazione finora
- 2007, Vol.40, Issues 5, The Professional VoiceDocumento269 pagine2007, Vol.40, Issues 5, The Professional VoiceLamia Bohliga100% (1)
- Laryngopharyngeal Reflux, DR A HaddadDocumento35 pagineLaryngopharyngeal Reflux, DR A HaddadLilia ScutelnicNessuna valutazione finora
- Interpreting Bravo PH StudiesDocumento16 pagineInterpreting Bravo PH StudiesLilia ScutelnicNessuna valutazione finora
- Campaign 1 - English For The Military StudentDocumento160 pagineCampaign 1 - English For The Military StudentLilia ScutelnicNessuna valutazione finora
- Characterization of Laryngopharyngeal Reflux in PDFDocumento5 pagineCharacterization of Laryngopharyngeal Reflux in PDFLilia ScutelnicNessuna valutazione finora
- Anatomy of Reflux A Growing Health Problem PDFDocumento10 pagineAnatomy of Reflux A Growing Health Problem PDFLilia ScutelnicNessuna valutazione finora
- Laryngeal Morphological Changes DueDocumento5 pagineLaryngeal Morphological Changes DueLilia ScutelnicNessuna valutazione finora
- Acid Reflux Treatment For Hoarseness (Review) PDFDocumento17 pagineAcid Reflux Treatment For Hoarseness (Review) PDFLilia ScutelnicNessuna valutazione finora
- Laryngitis From RefluxDocumento6 pagineLaryngitis From RefluxLilia ScutelnicNessuna valutazione finora
- Abnormal Endoscopic Pharyngeal and LaryngealDocumento7 pagineAbnormal Endoscopic Pharyngeal and LaryngealLilia ScutelnicNessuna valutazione finora
- Anatomy of Reflux A Growing Health Problem PDFDocumento10 pagineAnatomy of Reflux A Growing Health Problem PDFLilia ScutelnicNessuna valutazione finora
- Posterior Commissure of The Human Larynx Revisited PDFDocumento8 paginePosterior Commissure of The Human Larynx Revisited PDFLilia ScutelnicNessuna valutazione finora
- Anatomy of Reflux A Growing Health Problem PDFDocumento10 pagineAnatomy of Reflux A Growing Health Problem PDFLilia ScutelnicNessuna valutazione finora
- Acid Reflux Treatment For Hoarseness (Review)Documento17 pagineAcid Reflux Treatment For Hoarseness (Review)Lilia ScutelnicNessuna valutazione finora
- Laryng Reflux 090825 1Documento13 pagineLaryng Reflux 090825 1Syafiq IshakNessuna valutazione finora
- Acoustical Voice Measurements Did Change After Treatment inDocumento7 pagineAcoustical Voice Measurements Did Change After Treatment inLilia ScutelnicNessuna valutazione finora
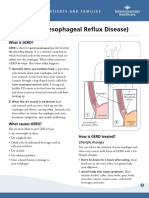
- Gastroesophageal Reflux Disease (GERD)Documento37 pagineGastroesophageal Reflux Disease (GERD)CraciunElenaNessuna valutazione finora
- Sulcus Vocalis AutosomnalDocumento6 pagineSulcus Vocalis AutosomnalLilia ScutelnicNessuna valutazione finora
- 1larynxma 121125054402 Phpapp01Documento73 pagine1larynxma 121125054402 Phpapp01Lilia ScutelnicNessuna valutazione finora
- Etiology of Vocal Fold Palsy 20060927Documento43 pagineEtiology of Vocal Fold Palsy 20060927Lilia ScutelnicNessuna valutazione finora
- Sulcus Vocalis 20070808Documento38 pagineSulcus Vocalis 20070808Lilia ScutelnicNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Pathophysiology Final Exam ReviewDocumento38 paginePathophysiology Final Exam ReviewBheru Lal100% (2)
- Pediatric Helicobacter Pylori Infection MedscapeDocumento6 paginePediatric Helicobacter Pylori Infection MedscapeRismawati AcenkNessuna valutazione finora
- NCM 116 Alterations in Nutri and GI Rev5Documento100 pagineNCM 116 Alterations in Nutri and GI Rev5JxshxzsNessuna valutazione finora
- GERD Gastroesophageal Reflux Disease Fact SheetDocumento2 pagineGERD Gastroesophageal Reflux Disease Fact SheetFatimah FadilahNessuna valutazione finora
- OmeprazoleDocumento2 pagineOmeprazoleJillian MendozaNessuna valutazione finora
- Brett Manning's Singing SuccessDocumento18 pagineBrett Manning's Singing Successgabi50% (2)
- RabeprazoleDocumento7 pagineRabeprazoleعبدالمحسن علي ENessuna valutazione finora
- Atrya BroucherDocumento5 pagineAtrya BroucherAkash SelokarNessuna valutazione finora
- MS Prelim Exam ReviewerDocumento9 pagineMS Prelim Exam ReviewerSheril100% (2)
- LPRDocumento29 pagineLPRrizky8Nessuna valutazione finora
- Esophagitis: Preferred By: Daryl S - AbrahamDocumento26 pagineEsophagitis: Preferred By: Daryl S - AbrahamBiway RegalaNessuna valutazione finora
- Gerd Gerd Gerd: Dr. Rocky Danilo Willis, M.D., AMTDocumento31 pagineGerd Gerd Gerd: Dr. Rocky Danilo Willis, M.D., AMTRocky Willis100% (1)
- DR Che Writing Correction Oet General NoteDocumento139 pagineDR Che Writing Correction Oet General NoteNitesh GandhiNessuna valutazione finora
- Esophageal Cancer NewDocumento52 pagineEsophageal Cancer Newapi-282115150Nessuna valutazione finora
- Hep & GIT Final MCQ 21 BDocumento23 pagineHep & GIT Final MCQ 21 BBaraa Elmasedy100% (3)
- Waking Up Gasping For Air Anxiety, Falling Asleep, Acid RefluxDocumento1 paginaWaking Up Gasping For Air Anxiety, Falling Asleep, Acid RefluxAstra CardinalNessuna valutazione finora
- Letters Combined (11 Referral, 2 Discharge, 1 Transfer)Documento49 pagineLetters Combined (11 Referral, 2 Discharge, 1 Transfer)Faisal ImtiazNessuna valutazione finora
- CaCO3 Drug StudDocumento2 pagineCaCO3 Drug StudAubrey SungaNessuna valutazione finora
- Nexpro Uae FinalDocumento13 pagineNexpro Uae Finalamr ahmedNessuna valutazione finora
- Usmle 01 1415 Manual DGDocumento55 pagineUsmle 01 1415 Manual DGMiguel Marcio Ortuño MejiaNessuna valutazione finora
- Esophageal Resection & Reconstruction: Yasser Elghoneimy M.DDocumento71 pagineEsophageal Resection & Reconstruction: Yasser Elghoneimy M.DFlaviu Ionuț FaurNessuna valutazione finora
- Sandhill Probes & CathetersDocumento2 pagineSandhill Probes & Catheterstadmur_tradingNessuna valutazione finora
- 2019 Dr. Sumarjo GerdDocumento18 pagine2019 Dr. Sumarjo GerdAnnisa Ayu NabilaNessuna valutazione finora
- Drug StudyDocumento4 pagineDrug StudyhsiriaNessuna valutazione finora
- Does Gastroesophageal Reflux Predispose To Rhinosinusitis? Predispone El Reflujo Gastroesofagico A Rinosinusitis?Documento31 pagineDoes Gastroesophageal Reflux Predispose To Rhinosinusitis? Predispone El Reflujo Gastroesofagico A Rinosinusitis?Victor EnachiNessuna valutazione finora
- Tiki Taka CK GastroenterologyDocumento9 pagineTiki Taka CK GastroenterologyDoc_mmaNessuna valutazione finora
- Gastrointestinal DisordersDocumento118 pagineGastrointestinal DisordersAhmad MakhloufNessuna valutazione finora
- Guidelines For The Surgical Treatment of Esophageal Achalasia PDFDocumento24 pagineGuidelines For The Surgical Treatment of Esophageal Achalasia PDFInomy ClaudiaNessuna valutazione finora
- 欧洲呼吸学会成人及儿童慢性咳嗽诊治指南Documento31 pagine欧洲呼吸学会成人及儿童慢性咳嗽诊治指南GaryNessuna valutazione finora
- MouthDocumento12 pagineMouthRodolfo MartinezNessuna valutazione finora