Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Scra 2014Documento3 pagineScra 2014Czara DyNessuna valutazione finora
- Marie Ivonne F. Reyes: Pasig Catholic SchoolDocumento1 paginaMarie Ivonne F. Reyes: Pasig Catholic SchoolCzara DyNessuna valutazione finora
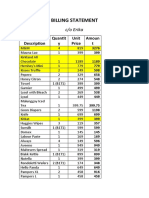
- S&R - Billing StatementDocumento4 pagineS&R - Billing StatementCzara DyNessuna valutazione finora
- Castillo vs. RepublicDocumento2 pagineCastillo vs. RepublicCzara DyNessuna valutazione finora
- Barcelote Vs - RepublicDocumento2 pagineBarcelote Vs - RepublicCzara DyNessuna valutazione finora
- Banking Mon 7718Documento2 pagineBanking Mon 7718Czara DyNessuna valutazione finora
- Corpo Notes 2018 PrelimsDocumento14 pagineCorpo Notes 2018 PrelimsCzara DyNessuna valutazione finora
- Institution of Heirs. It Will Not Result To IntestacyDocumento9 pagineInstitution of Heirs. It Will Not Result To IntestacyCzara DyNessuna valutazione finora
- Policarpio Vs Active BankDocumento2 paginePolicarpio Vs Active BankCzara DyNessuna valutazione finora
- G.R. No. L-48955, June 30, 1987)Documento8 pagineG.R. No. L-48955, June 30, 1987)Czara DyNessuna valutazione finora
- Sunio v. NLRCDocumento3 pagineSunio v. NLRCCzara DyNessuna valutazione finora
- Nil Cases FinalsDocumento37 pagineNil Cases FinalsCzara DyNessuna valutazione finora
- TORTS Page 2 Cases SyllabusDocumento77 pagineTORTS Page 2 Cases SyllabusCzara DyNessuna valutazione finora
- Annum From July 1, 2013 Until Full PaymentDocumento1 paginaAnnum From July 1, 2013 Until Full PaymentCzara DyNessuna valutazione finora
- Jimenez vs. FranciscoDocumento1 paginaJimenez vs. FranciscoCzara DyNessuna valutazione finora
- Q&A Wills Dean AligadaDocumento5 pagineQ&A Wills Dean AligadaCzara DyNessuna valutazione finora
- PNB Vs CA DigestDocumento3 paginePNB Vs CA DigestCzara DyNessuna valutazione finora
- Reynolds v. Ca (Dy)Documento2 pagineReynolds v. Ca (Dy)Czara DyNessuna valutazione finora
- Memorandum On Charter Change: Presidential Federal ConstitutionDocumento1 paginaMemorandum On Charter Change: Presidential Federal ConstitutionCzara DyNessuna valutazione finora
- Carpio CalaycayDocumento4 pagineCarpio CalaycayCzara DyNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Neuropathy EbookDocumento83 pagineNeuropathy EbookKristen ForsytheNessuna valutazione finora
- Neural Control and Co OrdinationDocumento16 pagineNeural Control and Co OrdinationDARSHAN KUMAR TNessuna valutazione finora
- Proprioception ReflexesDocumento20 pagineProprioception Reflexesthwiseman100% (1)
- Rate Coding and The Control of Muscle ForceDocumento12 pagineRate Coding and The Control of Muscle ForceMirna Liliana Carmona GarciaNessuna valutazione finora
- Human Physiology From Cells To Systems 9th Edition Sherwood Solutions ManualDocumento12 pagineHuman Physiology From Cells To Systems 9th Edition Sherwood Solutions ManualSamanthaStuartijgt100% (40)
- Laboratory Exercise 12Documento13 pagineLaboratory Exercise 12Jessa SuacitoNessuna valutazione finora
- BIO 2311 Lab Test 4 Study Guide Fall 2020Documento1 paginaBIO 2311 Lab Test 4 Study Guide Fall 2020Annabell CheungNessuna valutazione finora
- O-Levels Biology Definiton ListDocumento27 pagineO-Levels Biology Definiton ListOmar AdnanNessuna valutazione finora
- Nervous System WorksheetDocumento2 pagineNervous System WorksheetCamille Comas100% (2)
- Multiple-Choice Test Chapter 13: Coordination and Response: 1 A B C D 2 A B C D 3 A B C D 4 A B C DDocumento2 pagineMultiple-Choice Test Chapter 13: Coordination and Response: 1 A B C D 2 A B C D 3 A B C D 4 A B C DsybejoboNessuna valutazione finora
- Model Answers: Chapter 12 Coordination and Response in HumansDocumento5 pagineModel Answers: Chapter 12 Coordination and Response in HumansLaff IzzatulNessuna valutazione finora
- Chapter 4 Mechanism of Human BehaviorDocumento46 pagineChapter 4 Mechanism of Human BehaviorIsmaela BawicaNessuna valutazione finora
- Biology NotesDocumento102 pagineBiology Notesajabgul123493Nessuna valutazione finora
- PCP - Week 2 - QsDocumento4 paginePCP - Week 2 - Qsapi-502171898100% (1)
- NeuroDocumento162 pagineNeuroCindy ZhangNessuna valutazione finora
- Review For Test 3 - Anatomy & Physiology 2Documento7 pagineReview For Test 3 - Anatomy & Physiology 2fudgeboyNessuna valutazione finora
- The Nervous System: Dr. Garry NiedermayerDocumento74 pagineThe Nervous System: Dr. Garry Niedermayersweta paudelNessuna valutazione finora
- Selina Solutions For Class 10 Biology Chapter 10 The Nervous SystemDocumento13 pagineSelina Solutions For Class 10 Biology Chapter 10 The Nervous SystemKiyotaka AyanokoujiNessuna valutazione finora
- Anatomy and Physiology Midterm Chapter Quiz Nervous System and Special Senses Nervous SystemDocumento9 pagineAnatomy and Physiology Midterm Chapter Quiz Nervous System and Special Senses Nervous SystemMartin ManuelNessuna valutazione finora
- PHA 1.09 Intro To ANS ReyesDocumento9 paginePHA 1.09 Intro To ANS ReyesMichael Heinrich I. Santos100% (1)
- All About Nervous SystemDocumento35 pagineAll About Nervous SystemSophia AbrigoNessuna valutazione finora
- Muscular System Outline PDFDocumento102 pagineMuscular System Outline PDFAlok Singh100% (1)
- Isometric Exercise Induces Analgesia and Reduces Inhibition in Patellar TendinopathyDocumento8 pagineIsometric Exercise Induces Analgesia and Reduces Inhibition in Patellar TendinopathyVojtěch ŠmídNessuna valutazione finora
- Anatomy Unit Test Lumhs 2007Documento2 pagineAnatomy Unit Test Lumhs 2007Dr-Irfan HabibNessuna valutazione finora
- Coordination and Response PPT NotesDocumento137 pagineCoordination and Response PPT NotesANWESHA BAL100% (1)
- Special Senses NotesDocumento17 pagineSpecial Senses NotesataraxialliNessuna valutazione finora
- Edexcel IGCSE Biology AnswersDocumento36 pagineEdexcel IGCSE Biology AnswersSumiya Sultan70% (47)
- Nervous System WorksheetDocumento2 pagineNervous System WorksheetA. Nurul Virninda YusufNessuna valutazione finora
- Anatomy of Spinal Cord and Spinal Nerves, Reflexes, and Reaction Time and LearningDocumento32 pagineAnatomy of Spinal Cord and Spinal Nerves, Reflexes, and Reaction Time and LearningMickeyNessuna valutazione finora
- ANS DrugsDocumento82 pagineANS DrugsCrissan Jejomar AbanesNessuna valutazione finora