Potrebbero piacerti anche
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Guideline ITPDocumento11 pagineGuideline ITPRicho WijayaNessuna valutazione finora
- Cancer Prevention and Early DetectonDocumento64 pagineCancer Prevention and Early DetectonRicho WijayaNessuna valutazione finora
- Vitamin K Coagulopathy 2017Documento10 pagineVitamin K Coagulopathy 2017Richo WijayaNessuna valutazione finora
- Circumcision in HemophiliaDocumento11 pagineCircumcision in HemophiliaRicho WijayaNessuna valutazione finora
- Haemophilia and DentalDocumento8 pagineHaemophilia and DentalRicho WijayaNessuna valutazione finora
- Hypertonic Saline MythDocumento2 pagineHypertonic Saline MythRicho WijayaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- What Is A MicrodebriderDocumento7 pagineWhat Is A MicrodebriderIqbalur100% (1)
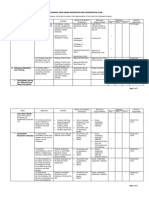
- For Companies - Sample - Three - Year Plan Matrix Revised 11.30.19Documento5 pagineFor Companies - Sample - Three - Year Plan Matrix Revised 11.30.19Arnold RadaNessuna valutazione finora
- Management of Patients With Burn Injury WEBDocumento28 pagineManagement of Patients With Burn Injury WEBJen Chua100% (2)
- Final Defense PowerpointDocumento10 pagineFinal Defense PowerpointPaul CrucisNessuna valutazione finora
- Peat PDFDocumento44 paginePeat PDFMary June Hayrelle Sale100% (2)
- IDT - 8 v1 Waste ManagementDocumento13 pagineIDT - 8 v1 Waste ManagementOzzyNessuna valutazione finora
- Muscolino - Narrazione Teatrale Del Sé e Riabilitazione PsichiatricaDocumento8 pagineMuscolino - Narrazione Teatrale Del Sé e Riabilitazione Psichiatricaamiramonti100Nessuna valutazione finora
- Mddo PhysicianshandbookDocumento88 pagineMddo Physicianshandbookmary engNessuna valutazione finora
- Setting Cleaning Validation Acceptance Limits For Topical FormulationsDocumento8 pagineSetting Cleaning Validation Acceptance Limits For Topical Formulationsvijayns_250355172Nessuna valutazione finora
- Hospital Medicine Maintenance of Certification Examination Blueprint - American Board of Internal MedicineDocumento4 pagineHospital Medicine Maintenance of Certification Examination Blueprint - American Board of Internal MedicineabimorgNessuna valutazione finora
- Building Self-Compassion - 03 - Preparing For Self-CompassionDocumento9 pagineBuilding Self-Compassion - 03 - Preparing For Self-CompassionThe Happy Mind HouseNessuna valutazione finora
- DavinciDocumento80 pagineDavinciVíctor GarcíaNessuna valutazione finora
- Treating The Mother of Black Triangles With Bioclear VeneersDocumento4 pagineTreating The Mother of Black Triangles With Bioclear VeneersThe Bioclear ClinicNessuna valutazione finora
- Fresofol 1 MCT-LCT PiDocumento18 pagineFresofol 1 MCT-LCT PiClaudia TiffanyNessuna valutazione finora
- DR - Kavita Priya Iicm 1Documento68 pagineDR - Kavita Priya Iicm 1Kavita PriyaNessuna valutazione finora
- Text A The Global Burden of DementiaDocumento25 pagineText A The Global Burden of DementianishantNessuna valutazione finora
- Discharge PlanDocumento2 pagineDischarge PlanJude Labajo100% (1)
- Resident Medical Officer KAmL4W116erDocumento4 pagineResident Medical Officer KAmL4W116erAman TyagiNessuna valutazione finora
- What Is Dricrimination?Documento2 pagineWhat Is Dricrimination?Shernan Paul ClaveriaNessuna valutazione finora
- Four Square Step TestDocumento2 pagineFour Square Step TestAnonymous igISmSUNessuna valutazione finora
- Nursing Care PlanDocumento4 pagineNursing Care Planjopearl1889% (9)
- Gestalt Transference PDFDocumento7 pagineGestalt Transference PDFAdriana Bogdanovska Toskic100% (2)
- CholecystectomyDocumento19 pagineCholecystectomyAlyssa Quilban MartinezNessuna valutazione finora
- Basic Hypnotherapy Steve G Jones EbookDocumento176 pagineBasic Hypnotherapy Steve G Jones EbookElias Calix87% (15)
- Pre Anesthetic Evaluation in DM - Liya AbrahamDocumento16 paginePre Anesthetic Evaluation in DM - Liya Abrahamvenky2430% (1)
- Nursing Care Plan (During Labor) : Subjective CuesDocumento5 pagineNursing Care Plan (During Labor) : Subjective CuesNatalie Antipolo100% (1)
- PWC Managing Innovation Pharma PDFDocumento20 paginePWC Managing Innovation Pharma PDFAryan RsNessuna valutazione finora
- Asphyxia NeonatorumDocumento35 pagineAsphyxia NeonatorumMuhammad RagilNessuna valutazione finora
- Synopsis Waste Water Treatment Via BioremediationDocumento35 pagineSynopsis Waste Water Treatment Via BioremediationManoj Meena100% (2)
- Biotech Bo SeriesDocumento2 pagineBiotech Bo SeriesArlinda Friyanti CallistaNessuna valutazione finora