Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Formulas From Epidemiology Kept Simple (3E) Chapter 3: Epidemiologic MeasuresDocumento7 pagineFormulas From Epidemiology Kept Simple (3E) Chapter 3: Epidemiologic MeasuresAnonymous dNeWZoQ100% (3)
- Dialysis Technician ExamsDocumento1 paginaDialysis Technician ExamstapanidepuNessuna valutazione finora
- Hemodialisis KdoqiDocumento183 pagineHemodialisis KdoqiMaFer WueRa100% (2)
- Top 10 Nephro Slides in Board ExamsDocumento223 pagineTop 10 Nephro Slides in Board ExamsMirza Shaharyar Baig100% (2)
- Pathophysiology (Chronic Renal Failure)Documento3 paginePathophysiology (Chronic Renal Failure)marshmalou86% (7)
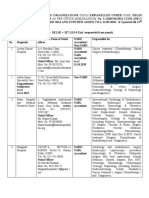
- Latest CGHS Panel Hospital List in Delhi 2022 PDFDocumento106 pagineLatest CGHS Panel Hospital List in Delhi 2022 PDFsatismisra7Nessuna valutazione finora
- New Ethical Review Submission FormDocumento9 pagineNew Ethical Review Submission FormKeshya Maleeza WeerakkodyNessuna valutazione finora
- Complications of Chronic Kidney Disease Current STDocumento32 pagineComplications of Chronic Kidney Disease Current STmetaNessuna valutazione finora
- Final KeysDocumento17 pagineFinal KeysKeshya Maleeza WeerakkodyNessuna valutazione finora
- Ms Public Health SampletestpaperDocumento3 pagineMs Public Health SampletestpaperKeshya Maleeza WeerakkodyNessuna valutazione finora
- Study DesignDocumento23 pagineStudy DesignKeshya Maleeza WeerakkodyNessuna valutazione finora
- Midterm KEY 2014Documento12 pagineMidterm KEY 2014SyafiqAziziNessuna valutazione finora
- Limits of AccuracyDocumento8 pagineLimits of AccuracyKeshya Maleeza WeerakkodyNessuna valutazione finora
- CancerEpi 5Documento19 pagineCancerEpi 5pr3etNessuna valutazione finora
- Final Exam 09Documento6 pagineFinal Exam 09Keshya Maleeza WeerakkodyNessuna valutazione finora
- Answers To TA Handout Questions For Exam 1Documento2 pagineAnswers To TA Handout Questions For Exam 1Keshya Maleeza WeerakkodyNessuna valutazione finora
- Slmaantibioticguidelines PDFDocumento147 pagineSlmaantibioticguidelines PDFKeshya Maleeza WeerakkodyNessuna valutazione finora
- CancerEpi 18 PDFDocumento21 pagineCancerEpi 18 PDFKeshya Maleeza WeerakkodyNessuna valutazione finora
- NephrologyDocumento12 pagineNephrologyKeshya Maleeza WeerakkodyNessuna valutazione finora
- RESEARCHDocumento46 pagineRESEARCHpreetie87Nessuna valutazione finora
- ADA Diabetes 2016 PDFDocumento61 pagineADA Diabetes 2016 PDFCésar P. SuárezNessuna valutazione finora
- Slmaantibioticguidelines PDFDocumento147 pagineSlmaantibioticguidelines PDFKeshya Maleeza WeerakkodyNessuna valutazione finora
- MCQ DiscussionDocumento1 paginaMCQ DiscussionKeshya Maleeza WeerakkodyNessuna valutazione finora
- 6229 23479 1 PBDocumento13 pagine6229 23479 1 PBKeshya Maleeza WeerakkodyNessuna valutazione finora
- Hyperkalaemia in AdultsDocumento13 pagineHyperkalaemia in AdultsKeshya Maleeza WeerakkodyNessuna valutazione finora
- Disability Policy PDFDocumento71 pagineDisability Policy PDFKeshya Maleeza WeerakkodyNessuna valutazione finora
- XMusculoskeleDocumento148 pagineXMusculoskeleKeshya Maleeza WeerakkodyNessuna valutazione finora
- KDIGO AKI Guideline DownloadDocumento141 pagineKDIGO AKI Guideline DownloadSandi AuliaNessuna valutazione finora
- Please Discuss The Following Conditions 1. Costocondritis. 2. Pneumothorax. 3.pulmonary Embolis. 4.acute Pericarditis. 5.tietez's SyndromeDocumento1 paginaPlease Discuss The Following Conditions 1. Costocondritis. 2. Pneumothorax. 3.pulmonary Embolis. 4.acute Pericarditis. 5.tietez's SyndromeKeshya Maleeza WeerakkodyNessuna valutazione finora
- Hyper Kala Emi ADocumento2 pagineHyper Kala Emi AKeshya Maleeza WeerakkodyNessuna valutazione finora
- MDLamawansaDocumento6 pagineMDLamawansaKeshya Maleeza WeerakkodyNessuna valutazione finora
- Sample Individual Income Statement & Balance SheetDocumento2 pagineSample Individual Income Statement & Balance Sheetsaorabh13Nessuna valutazione finora
- Sample Individual Income Statement & Balance SheetDocumento2 pagineSample Individual Income Statement & Balance Sheetsaorabh13Nessuna valutazione finora
- Training Course Programme FinalDocumento11 pagineTraining Course Programme FinalKeshya Maleeza WeerakkodyNessuna valutazione finora
- Abdominal X Rays Made Easy - CalcificationDocumento4 pagineAbdominal X Rays Made Easy - CalcificationMinh TanNessuna valutazione finora
- Padmashree Institute of Nursing: Vision and Mission StatementDocumento6 paginePadmashree Institute of Nursing: Vision and Mission StatementDr-Sanjay SinghaniaNessuna valutazione finora
- Cavsamir L Folder - 2022 - FADocumento2 pagineCavsamir L Folder - 2022 - FASanjay MehtaNessuna valutazione finora
- Pharmacokinetic Calculations Pharmacokinetic CalculationsDocumento1 paginaPharmacokinetic Calculations Pharmacokinetic CalculationsJoshua LaoNessuna valutazione finora
- Ultrasound of KidneyDocumento5 pagineUltrasound of KidneyMamunNessuna valutazione finora
- Estimation of Urea by DAM MethodDocumento3 pagineEstimation of Urea by DAM Methodmdanasd123Nessuna valutazione finora
- Diana Isabel Erazo SanchezDocumento20 pagineDiana Isabel Erazo SanchezWilhelmPatarroyoOliveraNessuna valutazione finora
- Medip, IJCP-2856 ODocumento6 pagineMedip, IJCP-2856 OMarcelita DuwiriNessuna valutazione finora
- Rapportrein2017 PDFDocumento382 pagineRapportrein2017 PDFShareDialysisNessuna valutazione finora
- 4800 Week 7 Renal StudentDocumento94 pagine4800 Week 7 Renal StudentLeAnna100% (1)
- Pengaruh Aromaterapi Inhalasi Terhadap Penurunan Nilai Kecemasan Pasien Gagal Ginjal Kronik Yang Menjalani HemodialisaDocumento6 paginePengaruh Aromaterapi Inhalasi Terhadap Penurunan Nilai Kecemasan Pasien Gagal Ginjal Kronik Yang Menjalani HemodialisaevangelineNessuna valutazione finora
- Acute Kidney InjuryDocumento3 pagineAcute Kidney InjuryHarkirat AtwalNessuna valutazione finora
- PDFDocumento18 paginePDFGene AngcaoNessuna valutazione finora
- Jay Fernando-Gaspar: Ms. Emilia P. Monicimpo, MD, MPH, CseeDocumento2 pagineJay Fernando-Gaspar: Ms. Emilia P. Monicimpo, MD, MPH, CseeGaspar De RosaNessuna valutazione finora
- Polyflux R Dialyzers Spec SheetDocumento2 paginePolyflux R Dialyzers Spec SheetShshank87100% (1)
- Sindroma Nefrotik DAFTAR PUSTAKADocumento3 pagineSindroma Nefrotik DAFTAR PUSTAKAEvi Dian PuspitaliseNessuna valutazione finora
- Nephrotic Syndrome: By: Yeni Ayu Prihastuti Moderator: DR. Dr. Hani Susianti, SP - PK (K)Documento42 pagineNephrotic Syndrome: By: Yeni Ayu Prihastuti Moderator: DR. Dr. Hani Susianti, SP - PK (K)yeniNessuna valutazione finora
- Management of Acute Kidney Injury in Children: Sri Lanka Journal of Child Health January 2019Documento6 pagineManagement of Acute Kidney Injury in Children: Sri Lanka Journal of Child Health January 2019HannaSaskiaIINessuna valutazione finora
- Systemic Lupus Erythematosus AssignmentDocumento6 pagineSystemic Lupus Erythematosus AssignmentnehaNessuna valutazione finora
- Chronic Kidney DiseaseDocumento7 pagineChronic Kidney DiseaseirmaNessuna valutazione finora
- Renal Pathology Unit ExamDocumento50 pagineRenal Pathology Unit ExamCherry RahimaNessuna valutazione finora
- Laporan Diagnosa ICD-ICDX Rawat Jalan - CompressedDocumento245 pagineLaporan Diagnosa ICD-ICDX Rawat Jalan - Compressedendang lestariNessuna valutazione finora
- Journal Pre-Proof: Advances in Chronic Kidney DiseaseDocumento19 pagineJournal Pre-Proof: Advances in Chronic Kidney DiseaseAbdul RokhmanNessuna valutazione finora
- Kidney Failure ThesisDocumento8 pagineKidney Failure Thesisafcngxbbx100% (3)
- Conn's DiseaseDocumento4 pagineConn's DiseaseMay Ann EsolanaNessuna valutazione finora