Potrebbero piacerti anche
- Diagnosis and Treatment of Worker-Related Musculoskeletal Disorders of The Upper Extremity OmbroDocumento705 pagineDiagnosis and Treatment of Worker-Related Musculoskeletal Disorders of The Upper Extremity OmbroDouglas GarciaNessuna valutazione finora
- Pharma Rapid Review FOCUSDocumento85 paginePharma Rapid Review FOCUSKeelNessuna valutazione finora
- 3.preoperative Patient Assessment and ManagementDocumento76 pagine3.preoperative Patient Assessment and Managementoliyad alemayehuNessuna valutazione finora
- Case StudyDocumento15 pagineCase StudyGaurav Kumar0% (1)
- 5 Reducing Time To Analgesia in The Emergency Department Using ADocumento10 pagine5 Reducing Time To Analgesia in The Emergency Department Using AMegaHandayaniNessuna valutazione finora
- Trauma Assessment Initial Trauma AssessmentDocumento5 pagineTrauma Assessment Initial Trauma AssessmentzulfahNessuna valutazione finora
- ER FINAL NOTES - CompressedDocumento68 pagineER FINAL NOTES - CompressedRosaree Mae PantojaNessuna valutazione finora
- Preop+++Goal Anaesthesia Record FormsDocumento5 paginePreop+++Goal Anaesthesia Record FormsShimelis AssefaNessuna valutazione finora
- History of Intramedullary NailsDocumento72 pagineHistory of Intramedullary NailsUhuebor DavidNessuna valutazione finora
- PacuDocumento93 paginePacunorhafizahstoh89Nessuna valutazione finora
- Toledo Code Blue PolicyDocumento4 pagineToledo Code Blue PolicySt SNessuna valutazione finora
- Please Read The Entire Form Carefully Before SigningDocumento2 paginePlease Read The Entire Form Carefully Before SigningKoh LudzNessuna valutazione finora
- Face Sheet, Patient Assessment & Reassessment, History, Physical Examination, Admission/Discharge RecordDocumento7 pagineFace Sheet, Patient Assessment & Reassessment, History, Physical Examination, Admission/Discharge RecordRonald Allan Valle SantosNessuna valutazione finora
- ICU Assessment Powerpoit Tuts1Documento25 pagineICU Assessment Powerpoit Tuts1Sharom SalasNessuna valutazione finora
- High Risk Consent For PCIDocumento1 paginaHigh Risk Consent For PCISree Sowjanya PatibandlaNessuna valutazione finora
- Anaphylaxis With Angioedema: Section I: Scenario DemographicsDocumento7 pagineAnaphylaxis With Angioedema: Section I: Scenario DemographicsharasthaNessuna valutazione finora
- FC Orth (SA) Intermediate Past Papers - 2012 Mar 28-3-2015Documento2 pagineFC Orth (SA) Intermediate Past Papers - 2012 Mar 28-3-2015Uhuebor DavidNessuna valutazione finora
- Emergency Severity Index Guidelines For Triage CeuDocumento71 pagineEmergency Severity Index Guidelines For Triage Ceuani mulyani100% (1)
- Preoperative Assessment PolicyDocumento10 paginePreoperative Assessment PolicymandayogNessuna valutazione finora
- Perioperative Scope of ServicesDocumento2 paginePerioperative Scope of Servicesmonir61Nessuna valutazione finora
- Early Warning Score & Rapid Response TeamDocumento26 pagineEarly Warning Score & Rapid Response TeamAsim IdreesNessuna valutazione finora
- DIC - RLE #4 For HemaDocumento12 pagineDIC - RLE #4 For HemaApril Mae Magos LabradorNessuna valutazione finora
- Pre Op 2010Documento37 paginePre Op 2010Tawona DhlakamaNessuna valutazione finora
- Pulseless VT/VF Algorithm First Impression: Sick or Not Sick? Primary SurveyDocumento9 paginePulseless VT/VF Algorithm First Impression: Sick or Not Sick? Primary SurveyBa LitNessuna valutazione finora
- Standardized Emergency Color CodesDocumento1 paginaStandardized Emergency Color CodesDivya ToppoNessuna valutazione finora
- FC Orth (SA) Intermediate Past Papers - 2012 Sept 28-3-2015Documento2 pagineFC Orth (SA) Intermediate Past Papers - 2012 Sept 28-3-2015Uhuebor DavidNessuna valutazione finora
- Perioperative Anticoagulation Bridging Guideline PostedDocumento6 paginePerioperative Anticoagulation Bridging Guideline PostedNuc Alexandru100% (1)
- GPH Admission BookletDocumento20 pagineGPH Admission BookletIndrawathan SamyNessuna valutazione finora
- Anthrax Clinical PathwayDocumento4 pagineAnthrax Clinical PathwayNeurologianak HarkitNessuna valutazione finora
- Post Cardiac Arrest CareDocumento20 paginePost Cardiac Arrest CareJayita Gayen Dutta100% (1)
- TransitionDocumento13 pagineTransitionDonna NituraNessuna valutazione finora
- Pre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIDocumento25 paginePre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIFatima MNessuna valutazione finora
- Neurological Examination PDFDocumento6 pagineNeurological Examination PDFArif K BashaNessuna valutazione finora
- Excretion and HomeostasisDocumento6 pagineExcretion and HomeostasisVernonNessuna valutazione finora
- 15Documento21 pagine15Tyson Easo JonesNessuna valutazione finora
- Documenting ConferringDocumento40 pagineDocumenting ConferringDidik Atmojo0% (1)
- Holistic Approach To HealthDocumento30 pagineHolistic Approach To Healthmaeydel0% (1)
- Emergency NursingDocumento15 pagineEmergency NursingAshley Ishika100% (1)
- Scripps Hospital Patient Visitor Policy PDFDocumento2 pagineScripps Hospital Patient Visitor Policy PDFcode4saleNessuna valutazione finora
- Blood Transfusion Single Use PathwayDocumento6 pagineBlood Transfusion Single Use PathwayropusanNessuna valutazione finora
- Assessment and Re-Assessment of Patients According To The Scope of ServiceDocumento9 pagineAssessment and Re-Assessment of Patients According To The Scope of Servicegiya nursingNessuna valutazione finora
- BSS 3rd Edition Participant Handbook CD FinalDocumento75 pagineBSS 3rd Edition Participant Handbook CD FinalUhuebor David100% (1)
- Emergency Drugs (LEAD)Documento8 pagineEmergency Drugs (LEAD)RayePrudenteNessuna valutazione finora
- ISE II ExampleDocumento23 pagineISE II Exampleanabenya86% (7)
- Truspected Stroke AlgorithmDocumento4 pagineTruspected Stroke Algorithmtri wahyunoNessuna valutazione finora
- Stroke Clinical PathwayDocumento1 paginaStroke Clinical PathwayKanoknun PisitpatcaragulNessuna valutazione finora
- Ed Assessment Tool SampleDocumento28 pagineEd Assessment Tool SampleAnonymous ibmeej9Nessuna valutazione finora
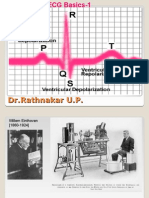
- ECG Basics 1Documento24 pagineECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNessuna valutazione finora
- Missing Patients ProcedureDocumento16 pagineMissing Patients ProcedureAgnieszka WaligóraNessuna valutazione finora
- Principles of Oncology and Outline of ManagementDocumento78 paginePrinciples of Oncology and Outline of ManagementPavan JonnadaNessuna valutazione finora
- Dirty Medicine by Lynne McTaggartDocumento4 pagineDirty Medicine by Lynne McTaggartNadia LakomkinaNessuna valutazione finora
- ACLS Protocols Pocket VersionDocumento2 pagineACLS Protocols Pocket Versionjohndoe1995Nessuna valutazione finora
- Data CollectionDocumento30 pagineData CollectionHarihara PuthiranNessuna valutazione finora
- Cordis Case Study PDFDocumento29 pagineCordis Case Study PDFsingh242Nessuna valutazione finora
- Define Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalDocumento15 pagineDefine Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalAbdul RahamanNessuna valutazione finora
- Measuring Up 2018Documento80 pagineMeasuring Up 2018CityNewsTorontoNessuna valutazione finora
- Post Anaesthesia Care Unit (Pacu) : DR - Shailendra.V.L. Specialist in AnaesthesiaDocumento29 paginePost Anaesthesia Care Unit (Pacu) : DR - Shailendra.V.L. Specialist in AnaesthesiatomasvainsteinNessuna valutazione finora
- JCI Standards Interpretation - June12004Documento18 pagineJCI Standards Interpretation - June12004Niharika SharmaNessuna valutazione finora
- 2 Critical Care UnitDocumento59 pagine2 Critical Care UnitPALMA , JULIA A.Nessuna valutazione finora
- Scape Vs FospeDocumento5 pagineScape Vs FospeDr. FarhanNessuna valutazione finora
- Enhancing Nurses Pain Assessment To Improve.11Documento2 pagineEnhancing Nurses Pain Assessment To Improve.11Na d'Nazaie CodeNessuna valutazione finora
- Module 9 Mechanical Ventilation PDFDocumento46 pagineModule 9 Mechanical Ventilation PDFChabboo SutabrataNessuna valutazione finora
- Massive Transfusion ProtocolDocumento11 pagineMassive Transfusion ProtocolAlaa Abdelmoaty OmranNessuna valutazione finora
- New MRD Manual 12-1-15Documento12 pagineNew MRD Manual 12-1-15aarti Hinge100% (1)
- L & M in Nursing - ConflictDocumento26 pagineL & M in Nursing - ConflictMichael SamaniegoNessuna valutazione finora
- Implementation Guidelines For The Canadian Emergency Department Triage & Acuity Scale (CTAS)Documento27 pagineImplementation Guidelines For The Canadian Emergency Department Triage & Acuity Scale (CTAS)Jery JsNessuna valutazione finora
- Critical Care SedationDa EverandCritical Care SedationAngelo Raffaele De GaudioNessuna valutazione finora
- ICU Scoring Systems A Complete Guide - 2020 EditionDa EverandICU Scoring Systems A Complete Guide - 2020 EditionNessuna valutazione finora
- Wound ManagementDocumento18 pagineWound ManagementUhuebor DavidNessuna valutazione finora
- Adrenal GlandDocumento9 pagineAdrenal GlandUhuebor DavidNessuna valutazione finora
- Essential Laboratory KnowledgeDocumento23 pagineEssential Laboratory KnowledgeUhuebor DavidNessuna valutazione finora
- (Open) Fractures: Potchefstroom Hopital OrthopedicsDocumento9 pagine(Open) Fractures: Potchefstroom Hopital OrthopedicsUhuebor DavidNessuna valutazione finora
- Biochemical Investigation of Renal FunctionDocumento34 pagineBiochemical Investigation of Renal FunctionUhuebor DavidNessuna valutazione finora
- Orthopaedic EmergenciesDocumento12 pagineOrthopaedic EmergenciesUhuebor DavidNessuna valutazione finora
- Abnormalities of The PuepriumDocumento14 pagineAbnormalities of The PuepriumUhuebor DavidNessuna valutazione finora
- Ankle FracturesDocumento13 pagineAnkle FracturesUhuebor DavidNessuna valutazione finora
- Meniscus Injuries: Uhuebor David Mbbs (Lagos)Documento23 pagineMeniscus Injuries: Uhuebor David Mbbs (Lagos)Uhuebor DavidNessuna valutazione finora
- The Intramedullary Nail Is Commonly Used For LongDocumento4 pagineThe Intramedullary Nail Is Commonly Used For LongUhuebor DavidNessuna valutazione finora
- Lower Limb AmputationDocumento37 pagineLower Limb AmputationUhuebor David0% (1)
- Surgery M&M 1Documento9 pagineSurgery M&M 1Uhuebor DavidNessuna valutazione finora
- Gallstone & Gallbladder Disease: DR Uhuebor DI MB, BS (Lagos)Documento16 pagineGallstone & Gallbladder Disease: DR Uhuebor DI MB, BS (Lagos)Uhuebor DavidNessuna valutazione finora
- Life Threatening, HIV ARV Related Medical Emergencies That Present To The EDDocumento13 pagineLife Threatening, HIV ARV Related Medical Emergencies That Present To The EDUhuebor DavidNessuna valutazione finora
- Etika Hub DR - PasienDocumento27 pagineEtika Hub DR - PasienJamali GagahNessuna valutazione finora
- 17A. Immune ToleranceDocumento8 pagine17A. Immune ToleranceEssington BeloNessuna valutazione finora
- 15 Plural FormsDocumento17 pagine15 Plural FormsRamuguhaNessuna valutazione finora
- Seed Coating) Damping OffDocumento11 pagineSeed Coating) Damping OffOlivia SimanungkalitNessuna valutazione finora
- Stress PDFDocumento7 pagineStress PDFGyanbitt KarNessuna valutazione finora
- Gastro Graf inDocumento12 pagineGastro Graf inquileuteNessuna valutazione finora
- Chlamydia Power PointDocumento19 pagineChlamydia Power PointAnne McfarlandNessuna valutazione finora
- MCQs Resuscitation BagDocumento2 pagineMCQs Resuscitation BagSaeedAliAl-shahtoor100% (1)
- 536 2 FullDocumento9 pagine536 2 Fullkiran shettyNessuna valutazione finora
- Strategic Group Minutes October 7th 2021 DraftDocumento10 pagineStrategic Group Minutes October 7th 2021 Draftapi-349611130Nessuna valutazione finora
- CPE239 Demonstration 411Documento11 pagineCPE239 Demonstration 411Hong Jun TeeNessuna valutazione finora
- Coconut Oil BenefitsDocumento2 pagineCoconut Oil BenefitsCharles Galan100% (1)
- Biomarkers-A General ReviewDocumento17 pagineBiomarkers-A General ReviewKevin FossNessuna valutazione finora
- Isolation of Endophytic Fungi From Artemisia Annua, L and Identification of Their Antimicrobial Compound Using Bioautography MethodDocumento5 pagineIsolation of Endophytic Fungi From Artemisia Annua, L and Identification of Their Antimicrobial Compound Using Bioautography MethodMuhammad ArismunandarNessuna valutazione finora
- Pe-4 GR12 2ndsem 3RDQ Module 3 W5W6Documento15 paginePe-4 GR12 2ndsem 3RDQ Module 3 W5W6Leslie Joy Yata MonteroNessuna valutazione finora
- Enoxaparin Sodium Manufacturer - Teena LabsDocumento3 pagineEnoxaparin Sodium Manufacturer - Teena Labsteena labsNessuna valutazione finora
- Nemeroff Et Al. 2013 - Dsm-5 2013 Collection Psychiatrist Views (Word Drop)Documento19 pagineNemeroff Et Al. 2013 - Dsm-5 2013 Collection Psychiatrist Views (Word Drop)DestriNessuna valutazione finora
- Golden Pearls of Gynecology and Obstetrics by DR Nadeem SHBDocumento10 pagineGolden Pearls of Gynecology and Obstetrics by DR Nadeem SHBusamaNessuna valutazione finora
- BBT423 L2Documento23 pagineBBT423 L2wowipev155Nessuna valutazione finora
- Sanna Labs PDFDocumento4 pagineSanna Labs PDFmudassarhasan786Nessuna valutazione finora
- Reading ComprehensionDocumento27 pagineReading ComprehensionNguyen MinhNessuna valutazione finora
- FastfoodDocumento13 pagineFastfoodapi-488116516Nessuna valutazione finora
- Toxicology of Cleaning AgentsDocumento38 pagineToxicology of Cleaning AgentsThe AbyssinicansNessuna valutazione finora
- Hypomagnesemic Tetany in Calve1Documento1 paginaHypomagnesemic Tetany in Calve1Morad ImadNessuna valutazione finora
- Massey Bedside ScreenDocumento1 paginaMassey Bedside ScreenAna Carolina Machuca100% (1)