Potrebbero piacerti anche
- Module 1 - Intro To OSHA (Student Handouts)Documento42 pagineModule 1 - Intro To OSHA (Student Handouts)memey grepo ramosNessuna valutazione finora
- Structures Failures Reasons and MitigationDa EverandStructures Failures Reasons and MitigationNessuna valutazione finora
- Introduction to OSHA Training HandoutsDocumento42 pagineIntroduction to OSHA Training HandoutsfodaozaoNessuna valutazione finora
- 2009 International Building Code Need to Know: The 20% of the Code You Need 80% of the Time: The 20% of the Code You Need 80% of the TimeDa Everand2009 International Building Code Need to Know: The 20% of the Code You Need 80% of the Time: The 20% of the Code You Need 80% of the TimeNessuna valutazione finora
- Sabic 3Documento5 pagineSabic 3Farrukh Javed0% (1)
- Spot Welding Interview Success: An Introduction to Spot WeldingDa EverandSpot Welding Interview Success: An Introduction to Spot WeldingNessuna valutazione finora
- Accident Report ElectDocumento8 pagineAccident Report Electapi-247438096Nessuna valutazione finora
- Chapter 1 Introduction DellDocumento21 pagineChapter 1 Introduction DellMuhd AkmalNessuna valutazione finora
- Health and Safety News - September 2009Documento33 pagineHealth and Safety News - September 2009HealthSafety100% (2)
- Feedstock Technology for Reactive Metal Injection Molding: Process, Design, and ApplicationDa EverandFeedstock Technology for Reactive Metal Injection Molding: Process, Design, and ApplicationNessuna valutazione finora
- Oil and Gas Well Drilling and Servicing Etool - Site Preparation - Site Preparation - Occupational Safety and Health AdministrationDocumento3 pagineOil and Gas Well Drilling and Servicing Etool - Site Preparation - Site Preparation - Occupational Safety and Health AdministrationMuhammad ZainNessuna valutazione finora
- Proposed Apartment Development in Kizingo: CorporationDocumento10 pagineProposed Apartment Development in Kizingo: Corporationmusiomi2005Nessuna valutazione finora
- 20 CasesDocumento10 pagine20 CasesEdmil Jhon AriquezNessuna valutazione finora
- Dokumen - Tips Building Technology Sba Adrian GreavesDocumento25 pagineDokumen - Tips Building Technology Sba Adrian Greavesdavaughn1450Nessuna valutazione finora
- Risk assessment implementation sheet analysisDocumento11 pagineRisk assessment implementation sheet analysisciafootNessuna valutazione finora
- Opening Process Equipment OPE Important Considerations Moloney ExxonMobil DCU FCCU SRU Budapest 2017Documento46 pagineOpening Process Equipment OPE Important Considerations Moloney ExxonMobil DCU FCCU SRU Budapest 2017maxadvanceNessuna valutazione finora
- TUTORIAL 1 Accident StatisticDocumento6 pagineTUTORIAL 1 Accident StatisticHafizuddin AdzharNessuna valutazione finora
- Cellar Reserve Pit: Potential HazardDocumento12 pagineCellar Reserve Pit: Potential HazardFriktNessuna valutazione finora
- Potential Hazard:: Cellar Reserve PitDocumento9 paginePotential Hazard:: Cellar Reserve PitFriktNessuna valutazione finora
- Al/Al O Metal Matrix Composites (MMCS) and Macrocomposites For Armor ApplicationsDocumento18 pagineAl/Al O Metal Matrix Composites (MMCS) and Macrocomposites For Armor ApplicationsMani KandanNessuna valutazione finora
- Nace 2019 13507Documento13 pagineNace 2019 13507Umair SarwarNessuna valutazione finora
- Lecture 5 - Health and Safety in ConstrutionDocumento54 pagineLecture 5 - Health and Safety in ConstrutionZain GhummanNessuna valutazione finora
- Sean C. Cronauer: EducationDocumento3 pagineSean C. Cronauer: EducationSean CronauerNessuna valutazione finora
- Week 3 (Human Factors)Documento3 pagineWeek 3 (Human Factors)AinaNessuna valutazione finora
- AL Solutions, Inc. Metal Dust Explosion and FireDocumento31 pagineAL Solutions, Inc. Metal Dust Explosion and FireSafety and Health magazineNessuna valutazione finora
- IGC 3 - Management Report - IGC 3 SampleDocumento4 pagineIGC 3 - Management Report - IGC 3 SampleHariKN68% (25)
- Braithwaite, J. W. & Buchheit, R. G. - Aspects of Two Corrosion Processes Relevant To Military Hardware (SANDIA REPORT, 1997)Documento28 pagineBraithwaite, J. W. & Buchheit, R. G. - Aspects of Two Corrosion Processes Relevant To Military Hardware (SANDIA REPORT, 1997)Luis Gustavo PachecoNessuna valutazione finora
- Technical English Level 4 Progress Test 6 (Units 11-12) : Answer All The QuestionsDocumento4 pagineTechnical English Level 4 Progress Test 6 (Units 11-12) : Answer All The QuestionsHuy HuyNessuna valutazione finora
- Roof Structural Assessment Report for Solar Panel InstallationDocumento9 pagineRoof Structural Assessment Report for Solar Panel InstallationTrader RedNessuna valutazione finora
- Mitigate Buried Pipeline CorrosionDocumento27 pagineMitigate Buried Pipeline Corrosionhitm357Nessuna valutazione finora
- Management Report SampleDocumento9 pagineManagement Report SampleMuhammadNessuna valutazione finora
- 091 Preventing Crown CollisionsDocumento5 pagine091 Preventing Crown CollisionsalduwaikiNessuna valutazione finora
- 2000-01 Manual A-C-Heater Systems Blazer, Jimmy, Sonoma - s10 PickupDocumento5 pagine2000-01 Manual A-C-Heater Systems Blazer, Jimmy, Sonoma - s10 PickupKidd100% (1)
- Annual Market Review & Forecast: Laser WeldingDocumento40 pagineAnnual Market Review & Forecast: Laser WeldingwwwpolNessuna valutazione finora
- T37 Lec04Documento7 pagineT37 Lec04bilalNessuna valutazione finora
- A New Technological Tool For Patching Asphalt PavementDocumento45 pagineA New Technological Tool For Patching Asphalt PavementSekely FeycohNessuna valutazione finora
- AAMA 320-10: General Guidelines For Troubleshooting Welded Thermoplastic CornersDocumento17 pagineAAMA 320-10: General Guidelines For Troubleshooting Welded Thermoplastic CornersDavidNessuna valutazione finora
- DFI-ADSC Micropile Guide Spec PDFDocumento0 pagineDFI-ADSC Micropile Guide Spec PDFmy09Nessuna valutazione finora
- No. 124 Movements of Tankers and Liquids Atthe Wrong Time or Intothe Wrong PlaceDocumento8 pagineNo. 124 Movements of Tankers and Liquids Atthe Wrong Time or Intothe Wrong PlaceLisa FosterNessuna valutazione finora
- MNMFatalAlert10222013 PDFDocumento1 paginaMNMFatalAlert10222013 PDFYos FontiniNessuna valutazione finora
- Lecturenotesmsc 2019Documento23 pagineLecturenotesmsc 2019chhoun boraNessuna valutazione finora
- Means and Methods for achieving Bovis Lend Lease Global Minimum RequirementsDocumento189 pagineMeans and Methods for achieving Bovis Lend Lease Global Minimum RequirementsAlex FirthNessuna valutazione finora
- Refinery Power Failures - Causes Costs and SolutionsDocumento14 pagineRefinery Power Failures - Causes Costs and SolutionsPradeep SinghNessuna valutazione finora
- AAMA 2603-2017aDocumento14 pagineAAMA 2603-2017acatseyesbabyNessuna valutazione finora
- The Magazine of ASMEDocumento68 pagineThe Magazine of ASMERahul SinghNessuna valutazione finora
- Near Miss Report NM SIN 025Documento15 pagineNear Miss Report NM SIN 025za8319712Nessuna valutazione finora
- OSG Rev3Documento39 pagineOSG Rev3y6d6pct9fyNessuna valutazione finora
- Barricades and Signage (04 19) - CS Energy RegisteredDocumento8 pagineBarricades and Signage (04 19) - CS Energy RegisteredANessuna valutazione finora
- Coursework 1 Stais Gkoumas 97.5%Documento26 pagineCoursework 1 Stais Gkoumas 97.5%dgNessuna valutazione finora
- Truck ManualDocumento67 pagineTruck Manualjohny eiji okadaNessuna valutazione finora
- Advanced Silicide Based Materials - MoSi2Documento13 pagineAdvanced Silicide Based Materials - MoSi2chandravadiyaketanNessuna valutazione finora
- Naukri Srinivasan (9y 0m)Documento3 pagineNaukri Srinivasan (9y 0m)anjana krishnanNessuna valutazione finora
- 777D CAT DETECTDocumento99 pagine777D CAT DETECTAlexis ContadorNessuna valutazione finora
- Gas Turbine Compressor IssuesDocumento9 pagineGas Turbine Compressor IssuesJJNessuna valutazione finora
- Metalized Film and Dyne LevelsDocumento10 pagineMetalized Film and Dyne Levelsfregil_64100% (1)
- 10 Yrs Mine FatalityDocumento20 pagine10 Yrs Mine FatalityChiranjib BanerjeeNessuna valutazione finora
- An Advanced Methodology For Windscreen MdellingDocumento10 pagineAn Advanced Methodology For Windscreen Mdellingbaca88Nessuna valutazione finora
- Hatfield Plaza - AB - Combined Floor Plan - Area A - TEMPLATEDocumento1 paginaHatfield Plaza - AB - Combined Floor Plan - Area A - TEMPLATEAndres Cedeno TutivenNessuna valutazione finora
- Dataflex Letters 170129300764Documento2 pagineDataflex Letters 170129300764Andres Cedeno TutivenNessuna valutazione finora
- Structural Sample DrawingDocumento1 paginaStructural Sample DrawingAndres Cedeno TutivenNessuna valutazione finora
- Second Floor PlanDocumento1 paginaSecond Floor PlanAndres Cedeno TutivenNessuna valutazione finora
- Concept DrawingsDocumento4 pagineConcept DrawingsAndres Cedeno TutivenNessuna valutazione finora
- BEXEL Manager-Getting StartedDocumento11 pagineBEXEL Manager-Getting StartedAndres Cedeno TutivenNessuna valutazione finora
- House PhotosDocumento16 pagineHouse PhotosAndres Cedeno TutivenNessuna valutazione finora
- Framing Work Block Done - Rev CDocumento3 pagineFraming Work Block Done - Rev CAndres Cedeno TutivenNessuna valutazione finora
- BIM NamingDocumento8 pagineBIM NamingAndres Cedeno TutivenNessuna valutazione finora
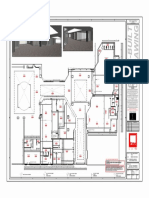
- 1/8" 1'-0" 1 01 First Floor HVAC Ceiling PlanDocumento10 pagine1/8" 1'-0" 1 01 First Floor HVAC Ceiling PlanAndres Cedeno TutivenNessuna valutazione finora
- Building ModelsDocumento1 paginaBuilding ModelsAndres Cedeno TutivenNessuna valutazione finora
- Dipanel Galvalume PDFDocumento1 paginaDipanel Galvalume PDFAndres Cedeno TutivenNessuna valutazione finora
- Window Door SchedulesDocumento1 paginaWindow Door SchedulesAndres Cedeno TutivenNessuna valutazione finora
- 1976 - House Technical Drawings PDFDocumento5 pagine1976 - House Technical Drawings PDFAndres Cedeno TutivenNessuna valutazione finora
- CI1697-R - Bridge Modeling Approaches HandoutDocumento22 pagineCI1697-R - Bridge Modeling Approaches HandoutAndres Cedeno TutivenNessuna valutazione finora
- Document E202 - 2008: Building Information Modeling Protocol ExhibitDocumento9 pagineDocument E202 - 2008: Building Information Modeling Protocol ExhibitAndres Cedeno TutivenNessuna valutazione finora
- Aiming For Continuous Flow: LCI White Paper-3 March 5, 1999 Glenn Ballard and Iris Tommelein, LCIDocumento6 pagineAiming For Continuous Flow: LCI White Paper-3 March 5, 1999 Glenn Ballard and Iris Tommelein, LCIAndres Cedeno TutivenNessuna valutazione finora
- Dipanel Galvalume PDFDocumento1 paginaDipanel Galvalume PDFAndres Cedeno TutivenNessuna valutazione finora
- Lean Project Delivery SystemDocumento7 pagineLean Project Delivery SystemSebastian BernalNessuna valutazione finora
- 05 Positive Vs Negative Iteration in DesignDocumento12 pagine05 Positive Vs Negative Iteration in DesignMelvin MolinaNessuna valutazione finora
- Cedeno - Final Model LogDocumento5 pagineCedeno - Final Model LogAndres Cedeno TutivenNessuna valutazione finora
- Cedeno - Assignment - L10 - Sheet - A103 - East and West ElevationsDocumento1 paginaCedeno - Assignment - L10 - Sheet - A103 - East and West ElevationsAndres Cedeno TutivenNessuna valutazione finora
- Research AssignmentDocumento3 pagineResearch AssignmentAndres Cedeno TutivenNessuna valutazione finora
- LCI Glossary01152014 PDFDocumento7 pagineLCI Glossary01152014 PDFAndres Cedeno TutivenNessuna valutazione finora
- Applying Lean Construction To Loss Control: Xavier BriosoDocumento11 pagineApplying Lean Construction To Loss Control: Xavier BriosoLuis Fernando Cruzalegui BonillaNessuna valutazione finora
- Koskela-Application of The New Production Philosophy To CosntructionDocumento81 pagineKoskela-Application of The New Production Philosophy To CosntructionlmonteroNessuna valutazione finora
- Last Planner SystemDocumento192 pagineLast Planner SystemJose Stein GuerreroNessuna valutazione finora
- Research AssignmentDocumento3 pagineResearch AssignmentAndres Cedeno TutivenNessuna valutazione finora
- Last Planner SystemDocumento192 pagineLast Planner SystemJose Stein GuerreroNessuna valutazione finora
- Introduction To Project Planning - Bus Stop Case StudyDocumento28 pagineIntroduction To Project Planning - Bus Stop Case StudyAndres Cedeno TutivenNessuna valutazione finora
- BCSA - 36 04 Secure PDFDocumento50 pagineBCSA - 36 04 Secure PDFWilliam CaballeroNessuna valutazione finora
- Hempel Topaz SG Enamel 524ME MsdsDocumento10 pagineHempel Topaz SG Enamel 524ME MsdsM.FAIZAN ARSHADNessuna valutazione finora
- HSE IMS System ManualDocumento172 pagineHSE IMS System Manualdzelig0% (1)
- Module 4 - Housekeeping (Occupational Safety)Documento20 pagineModule 4 - Housekeeping (Occupational Safety)Sam100% (1)
- Chieftain 1400 Operations Manual Revision 3.4 (English) - 1Documento434 pagineChieftain 1400 Operations Manual Revision 3.4 (English) - 1Steven Dolan88% (8)
- EHS Manual - FinalDocumento53 pagineEHS Manual - Finalanoushia alviNessuna valutazione finora
- Savlon CairDocumento2 pagineSavlon CairMelly SawitriNessuna valutazione finora
- SDS Safety Data SheetDocumento6 pagineSDS Safety Data SheetRossel CruzNessuna valutazione finora
- Ms Prathmesh Construction ProfileDocumento20 pagineMs Prathmesh Construction ProfilePratik KharmateNessuna valutazione finora
- Vikarant Institute of Technology & Management: Internship Project Report Prepared atDocumento26 pagineVikarant Institute of Technology & Management: Internship Project Report Prepared atVarunNessuna valutazione finora
- Disaster Management Plan for DISH OfficeDocumento14 pagineDisaster Management Plan for DISH Officebombonde_797469Nessuna valutazione finora
- P Langu D&P Sys 9&C101 GHS Eu&c888 Profopen&c200 True&c001 MSDS&C002 Reg Eu&c003 E&c005 500000001177&C013 1112495Documento15 pagineP Langu D&P Sys 9&C101 GHS Eu&c888 Profopen&c200 True&c001 MSDS&C002 Reg Eu&c003 E&c005 500000001177&C013 1112495Hewa PCNessuna valutazione finora
- Occupational Health & Safety at Work Attachment Report.Documento34 pagineOccupational Health & Safety at Work Attachment Report.Clyde K. Lesole100% (5)
- 54L EutectrodeDocumento9 pagine54L EutectrodeJuan LondonoNessuna valutazione finora
- Legal Register To UseDocumento8 pagineLegal Register To UseKingsley Ahanonu67% (3)
- Epikuron 100 G MSDSDocumento9 pagineEpikuron 100 G MSDSIbad MuhammedNessuna valutazione finora
- Health and Safety Check CateringDocumento5 pagineHealth and Safety Check CateringDayang Sari AndrianiNessuna valutazione finora
- Nursing Assistance L3Documento117 pagineNursing Assistance L3MaxNessuna valutazione finora
- IG1 Element 2Documento30 pagineIG1 Element 2Shah Wali UllahNessuna valutazione finora
- Blue Horizon Evacuation Procedures Toolbox TalkDocumento3 pagineBlue Horizon Evacuation Procedures Toolbox Talkklaus jensenNessuna valutazione finora
- P1 Describe The Potential Business Opportunities For A Micro-Business Start-UpDocumento32 pagineP1 Describe The Potential Business Opportunities For A Micro-Business Start-UpRabi rabiNessuna valutazione finora
- Procedure For Communication, Participation and ConsultationDocumento3 pagineProcedure For Communication, Participation and ConsultationDaniel Cheng MahsaNessuna valutazione finora
- Permit To Work Course OutlineDocumento6 paginePermit To Work Course Outlineafiwhyber100% (2)
- OTIS RISK ASSESSMENT FORMDocumento1 paginaOTIS RISK ASSESSMENT FORMeduardoNessuna valutazione finora
- Training Regulations Bread and Pastry Production NC Ii Productiontraining RegulationsDocumento25 pagineTraining Regulations Bread and Pastry Production NC Ii Productiontraining Regulationskaye maleNessuna valutazione finora
- Factories Act Karnataka Rules 1948Documento140 pagineFactories Act Karnataka Rules 1948Guru Vaga75% (4)
- Ethanol Ahyd Histo 4lDocumento10 pagineEthanol Ahyd Histo 4lGeorge GrandinettiNessuna valutazione finora
- JSA Aircond Ducting WorkDocumento1 paginaJSA Aircond Ducting WorkRashidi Rahman100% (4)
- 02 04 AMM Daily HSE Statistics Report AprDocumento1 pagina02 04 AMM Daily HSE Statistics Report AprPT. ANUGRAH MIRAN MANDIRINessuna valutazione finora
- Heat Transfer Rajput SolutionDocumento6 pagineHeat Transfer Rajput SolutionBanbona AlkurdshNessuna valutazione finora
- A Poison Like No Other: How Microplastics Corrupted Our Planet and Our BodiesDa EverandA Poison Like No Other: How Microplastics Corrupted Our Planet and Our BodiesValutazione: 5 su 5 stelle5/5 (1)
- The Invisible Rainbow: A History of Electricity and LifeDa EverandThe Invisible Rainbow: A History of Electricity and LifeValutazione: 4.5 su 5 stelle4.5/5 (21)
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsDa EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNessuna valutazione finora
- Introduction to Petroleum Process SafetyDa EverandIntroduction to Petroleum Process SafetyValutazione: 3 su 5 stelle3/5 (2)
- Nobody Cares: The Story of the World from SafetymanDa EverandNobody Cares: The Story of the World from SafetymanNessuna valutazione finora
- LNG Risk Based Safety: Modeling and Consequence AnalysisDa EverandLNG Risk Based Safety: Modeling and Consequence AnalysisNessuna valutazione finora
- Chemical Process Safety: Learning from Case HistoriesDa EverandChemical Process Safety: Learning from Case HistoriesValutazione: 4 su 5 stelle4/5 (14)
- Guidelines for Implementing Process Safety ManagementDa EverandGuidelines for Implementing Process Safety ManagementNessuna valutazione finora
- Incidents That Define Process SafetyDa EverandIncidents That Define Process SafetyNessuna valutazione finora
- Inherently Safer Chemical Processes: A Life Cycle ApproachDa EverandInherently Safer Chemical Processes: A Life Cycle ApproachValutazione: 5 su 5 stelle5/5 (1)
- Rules of Thumb for Maintenance and Reliability EngineersDa EverandRules of Thumb for Maintenance and Reliability EngineersValutazione: 4.5 su 5 stelle4.5/5 (12)
- Radium Girls: Women and Industrial Health Reform, 1910-1935Da EverandRadium Girls: Women and Industrial Health Reform, 1910-1935Valutazione: 4.5 su 5 stelle4.5/5 (4)
- Trevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationDa EverandTrevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationNessuna valutazione finora
- Safety Fundamentals and Best Practices in Construction IndustryDa EverandSafety Fundamentals and Best Practices in Construction IndustryNessuna valutazione finora
- Guidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisDa EverandGuidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisValutazione: 5 su 5 stelle5/5 (1)
- Practical Industrial Safety, Risk Assessment and Shutdown SystemsDa EverandPractical Industrial Safety, Risk Assessment and Shutdown SystemsValutazione: 4 su 5 stelle4/5 (11)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeDa EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNessuna valutazione finora
- Guidelines for Auditing Process Safety Management SystemsDa EverandGuidelines for Auditing Process Safety Management SystemsNessuna valutazione finora
- 3D Printing of Concrete: State of the Art and Challenges of the Digital Construction RevolutionDa Everand3D Printing of Concrete: State of the Art and Challenges of the Digital Construction RevolutionArnaud PerrotNessuna valutazione finora
- Safety and Intelligent Transport Systems Development in the People’s Republic of ChinaDa EverandSafety and Intelligent Transport Systems Development in the People’s Republic of ChinaNessuna valutazione finora
- A Complete Guide to Safety Officer Interview Questions and AnswersDa EverandA Complete Guide to Safety Officer Interview Questions and AnswersValutazione: 4 su 5 stelle4/5 (1)
- The Single Cure: Human Life Extension to 300+ YearsDa EverandThe Single Cure: Human Life Extension to 300+ YearsNessuna valutazione finora
- Exercise, Sport, and Bioanalytical Chemistry: Principles and PracticeDa EverandExercise, Sport, and Bioanalytical Chemistry: Principles and PracticeNessuna valutazione finora
- Safety Critical Systems Handbook: A Straight forward Guide to Functional Safety, IEC 61508 (2010 EDITION) and Related Standards, Including Process IEC 61511 and Machinery IEC 62061 and ISO 13849Da EverandSafety Critical Systems Handbook: A Straight forward Guide to Functional Safety, IEC 61508 (2010 EDITION) and Related Standards, Including Process IEC 61511 and Machinery IEC 62061 and ISO 13849Valutazione: 4 su 5 stelle4/5 (5)
- Electrical Safety Code Manual: A Plain Language Guide to National Electrical Code, OSHA and NFPA 70EDa EverandElectrical Safety Code Manual: A Plain Language Guide to National Electrical Code, OSHA and NFPA 70EValutazione: 3 su 5 stelle3/5 (6)
- One Health: Integrated Approach to 21st Century Challenges to HealthDa EverandOne Health: Integrated Approach to 21st Century Challenges to HealthJoana C. PrataNessuna valutazione finora
- Fire Protection Engineering in Building DesignDa EverandFire Protection Engineering in Building DesignValutazione: 4.5 su 5 stelle4.5/5 (5)