Potrebbero piacerti anche
- Cardiovascular System Anatomy and PhysiologyDocumento24 pagineCardiovascular System Anatomy and PhysiologyCandice100% (1)
- NURS02-Assessment of The Musculoskeletal SystemDocumento129 pagineNURS02-Assessment of The Musculoskeletal SystemAlec AnonNessuna valutazione finora
- Assessment of Musculoskeletal SystemDocumento12 pagineAssessment of Musculoskeletal SystemDina Thomas100% (6)
- CLG856H Wheel LoaderDocumento816 pagineCLG856H Wheel LoaderAli Kuncoro100% (1)
- Nursing BulletsDocumento123 pagineNursing BulletsCarmela MayNessuna valutazione finora
- Musculoskeletal MED SURGDocumento57 pagineMusculoskeletal MED SURGlolo0880Nessuna valutazione finora
- Integumentary SystemDocumento7 pagineIntegumentary Systemkuroko tetsuya100% (2)
- Central Nervous System PDFDocumento11 pagineCentral Nervous System PDFbilal officalNessuna valutazione finora
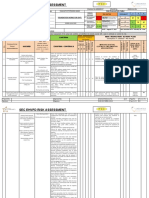
- SEC-EHV-Risk-assesment-form-Rev.-2..Foundation Works For OHTLDocumento4 pagineSEC-EHV-Risk-assesment-form-Rev.-2..Foundation Works For OHTLSn AhsanNessuna valutazione finora
- Integumentary SystemDocumento16 pagineIntegumentary Systemshenric16100% (7)
- Ppe Training NTTFDocumento47 paginePpe Training NTTFAkshatha M100% (1)
- Classification of FracturesDocumento26 pagineClassification of FracturesHoney May Rollan VicenteNessuna valutazione finora
- Medical Surgical Nursing PinoyDocumento85 pagineMedical Surgical Nursing PinoyrosebaseNessuna valutazione finora
- Range of Joint Motion Evaluation Chart OK PDFDocumento2 pagineRange of Joint Motion Evaluation Chart OK PDFcesamav100% (4)
- Disorders of The Genitourinary SystemDocumento49 pagineDisorders of The Genitourinary SystemYemaya84Nessuna valutazione finora
- Skeletal System: - Composed of The Body's Bones and Associated Ligaments, Tendons, and Cartilages. - FunctionsDocumento66 pagineSkeletal System: - Composed of The Body's Bones and Associated Ligaments, Tendons, and Cartilages. - FunctionsDenver TanhuanNessuna valutazione finora
- Musculoskeletal DISORDERSDocumento6 pagineMusculoskeletal DISORDERSJoe Stewart100% (1)
- Examination of Hip JointDocumento8 pagineExamination of Hip JointRebecca WongNessuna valutazione finora
- Skeletal Muscle Cells and Muscle Fiber FasciclesDocumento9 pagineSkeletal Muscle Cells and Muscle Fiber Fasciclesjessa prendol100% (1)
- CardiomyopathyDocumento2 pagineCardiomyopathyBianca SarmientoNessuna valutazione finora
- Focused Abdominal Sonography in Trauma (FAST)Documento56 pagineFocused Abdominal Sonography in Trauma (FAST)RannyNessuna valutazione finora
- Muscular System Anatomy and PhysiologyDocumento9 pagineMuscular System Anatomy and PhysiologyMichelle Tamor100% (1)
- Endocrine SystemDocumento8 pagineEndocrine Systemtheglobalnursing80% (5)
- Musculoskeletal AssessmentDocumento9 pagineMusculoskeletal AssessmentVincent John FallerNessuna valutazione finora
- Podiatry: Why Is It Important ?Documento5 paginePodiatry: Why Is It Important ?arunmptNessuna valutazione finora
- Musculoskeletal disorders in childrenDocumento73 pagineMusculoskeletal disorders in childrenMuhammadNessuna valutazione finora
- Care of Clients with BurnsDocumento3 pagineCare of Clients with BurnsROBERT C. REÑA, BSN, RN, MAN (ue)67% (3)
- Testing Cranial Nerves Activity SheetDocumento5 pagineTesting Cranial Nerves Activity Sheetapi-460447962Nessuna valutazione finora
- Neurologic AssessmentDocumento29 pagineNeurologic AssessmentJoessel_Marie__8991100% (1)
- Hematological Alterations: Disseminated Intravascular Coagulation (DIC)Documento16 pagineHematological Alterations: Disseminated Intravascular Coagulation (DIC)jhommmmmNessuna valutazione finora
- Lecture Guide Assessment-Of-Musculoskeletal-Function HPDocumento85 pagineLecture Guide Assessment-Of-Musculoskeletal-Function HPBlessed GarcianoNessuna valutazione finora
- Cardiovascular System - ReviewerDocumento11 pagineCardiovascular System - ReviewerEva Marie GaaNessuna valutazione finora
- Elbow Joint Injuries - Assessment & TreatmentDocumento55 pagineElbow Joint Injuries - Assessment & TreatmentSushma ImmadiNessuna valutazione finora
- Musculoskeletal System NotesDocumento114 pagineMusculoskeletal System Notesjenm1228100% (1)
- EndocrineDocumento12 pagineEndocrineAna FelNessuna valutazione finora
- Introduction To General AnatomyDocumento7 pagineIntroduction To General AnatomyPia Abila100% (1)
- Orthopedic NursingDocumento237 pagineOrthopedic Nursingɹǝʍdןnos100% (24)
- Balance Skeletal Traction1Documento31 pagineBalance Skeletal Traction1Maria Victoria ColomaNessuna valutazione finora
- Blood Transfusion and Blood ProductsDocumento7 pagineBlood Transfusion and Blood ProductsKatherine 'Chingboo' Leonico Laud100% (1)
- Neuroanatomy Questions GuideDocumento19 pagineNeuroanatomy Questions GuideGoNessuna valutazione finora
- Foot Reflexology Complete How To Techniques & Step by Step Instructions!Documento10 pagineFoot Reflexology Complete How To Techniques & Step by Step Instructions!Tony MickensNessuna valutazione finora
- Respiratory System Disorders R/T NursingDocumento27 pagineRespiratory System Disorders R/T NursinggakuiNessuna valutazione finora
- Nursing care of musculoskeletal disorders in childrenDocumento180 pagineNursing care of musculoskeletal disorders in childrenRiccyNessuna valutazione finora
- MusculoSkeletal SystemDocumento56 pagineMusculoSkeletal Systemmaj71% (7)
- Assessing Musculoskeletal (MSK) SystemDocumento8 pagineAssessing Musculoskeletal (MSK) SystemKeren GaciasNessuna valutazione finora
- Assessment of the Musculoskeletal SystemDocumento61 pagineAssessment of the Musculoskeletal Systemjoreynee100% (3)
- Eyes and Ears DisordersDocumento36 pagineEyes and Ears Disordersjeshema100% (4)
- Chapter 6 Bone Tissue 2304Documento37 pagineChapter 6 Bone Tissue 2304Sav Oli100% (1)
- The Gastro-Intestinal SystemDocumento12 pagineThe Gastro-Intestinal SystemRenelyn ComiaNessuna valutazione finora
- Human Sexuality: Concepts, Definitions, Anatomy & PhysiologyDocumento133 pagineHuman Sexuality: Concepts, Definitions, Anatomy & PhysiologyRick100% (1)
- D.muscular System PDFDocumento8 pagineD.muscular System PDFJohn Lawrence YbanezNessuna valutazione finora
- OrthoDocumento9 pagineOrthoFaith Levi Alecha AlferezNessuna valutazione finora
- Peripheral Vascular Disease NursingDocumento13 paginePeripheral Vascular Disease NursingCatlyn Chatpman100% (1)
- Badminton Drop Shot SkillDocumento6 pagineBadminton Drop Shot SkillChristine RidosNessuna valutazione finora
- Care of Patients with Musculoskeletal IssuesDocumento3 pagineCare of Patients with Musculoskeletal IssuesBryan Mae H. DegorioNessuna valutazione finora
- The Musculoskeletal SystemDocumento27 pagineThe Musculoskeletal SystemEduardoAlejoZamoraJr.Nessuna valutazione finora
- Endocrine DisordersDocumento3 pagineEndocrine DisordersIrish OrleansNessuna valutazione finora
- The Balanced Skeletal TractionDocumento1 paginaThe Balanced Skeletal TractionGemarie Adarlo CastilloNessuna valutazione finora
- Common Musculoskeletal Problems: DefinedDocumento17 pagineCommon Musculoskeletal Problems: DefinedAllean Sarmiento ApolinarioNessuna valutazione finora
- Musculoskeletal Note1Documento34 pagineMusculoskeletal Note1FreeNursingNotes100% (4)
- Assist With Client or Patient MovementDocumento88 pagineAssist With Client or Patient Movementmihret gashayeNessuna valutazione finora
- 6 Assessment of The Thorax and LungsDocumento6 pagine6 Assessment of The Thorax and LungsFreisanChenMandumotan100% (1)
- Muscular SystemDocumento4 pagineMuscular Systemquosha2Nessuna valutazione finora
- Cardiovascular 4416Documento5 pagineCardiovascular 4416api-3703191Nessuna valutazione finora
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDa EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNessuna valutazione finora
- Musculoskeletal System-Topic 8Documento40 pagineMusculoskeletal System-Topic 8Heba TabchNessuna valutazione finora
- It 2 - Pengantar Kartilago, Otot, Dan Tulang (Irw)Documento48 pagineIt 2 - Pengantar Kartilago, Otot, Dan Tulang (Irw)RurieAwaliaSuhardiNessuna valutazione finora
- Sistem Muskuloskeletal: 3 September 2019Documento45 pagineSistem Muskuloskeletal: 3 September 2019HafshahNessuna valutazione finora
- Bone Structure and Function in 40 CharactersDocumento24 pagineBone Structure and Function in 40 CharactersDioNessuna valutazione finora
- MIDTERMS AnatomyDocumento6 pagineMIDTERMS AnatomyCHIKA IN A MINUTENessuna valutazione finora
- How the Eye Works and What is GlaucomaDocumento34 pagineHow the Eye Works and What is GlaucomaNanik Herlina MarwanNessuna valutazione finora
- Dutchess County: Traffic Safety DataDocumento30 pagineDutchess County: Traffic Safety DataDaily FreemanNessuna valutazione finora
- Asda-A2 M en 20100429Documento517 pagineAsda-A2 M en 20100429Mario Plinio CrivelliNessuna valutazione finora
- Hojo Undo 2Documento3 pagineHojo Undo 2danevide100% (1)
- Mammal Skeleton Functions & RegionsDocumento19 pagineMammal Skeleton Functions & RegionsPenelope May MorkelNessuna valutazione finora
- List of Anatomy Mnemonics - WikipediaDocumento33 pagineList of Anatomy Mnemonics - WikipediaSudeepthiNessuna valutazione finora
- Distal Radius Fractures With Ulnar Styloid Fracture - V2Documento30 pagineDistal Radius Fractures With Ulnar Styloid Fracture - V2Chinmaye PurushothamNessuna valutazione finora
- Bromhidrosis NdyagDocumento5 pagineBromhidrosis Ndyagika_anggrainiNessuna valutazione finora
- Burn WoundsDocumento14 pagineBurn WoundsRuxandra BadiuNessuna valutazione finora
- MegaTraveller House Rules IIDocumento37 pagineMegaTraveller House Rules IIDavid FoleyNessuna valutazione finora
- Harry Potter SpellsDocumento21 pagineHarry Potter SpellsSotiris Pappas100% (1)
- 1 Personal SafetyDocumento2 pagine1 Personal SafetyVladNessuna valutazione finora
- Orthotics and Prosthetics LectureDocumento40 pagineOrthotics and Prosthetics LectureRock Obaidat100% (1)
- Burn Injury: Dr. Miguel Johnson Mbbs Mrcsed Plastic Surgery Resident University of The West Indies JamaicaDocumento21 pagineBurn Injury: Dr. Miguel Johnson Mbbs Mrcsed Plastic Surgery Resident University of The West Indies JamaicaMiguelito JohnsonNessuna valutazione finora
- Cartilage Forming TumorsDocumento10 pagineCartilage Forming TumorsRavikiran NandirajuNessuna valutazione finora
- Skeletal System QuestionsDocumento44 pagineSkeletal System QuestionsSritama GhoshNessuna valutazione finora
- Chest Drains GuidanceDocumento14 pagineChest Drains Guidancenob2011nobNessuna valutazione finora
- GRDA Intro Bony PelvisDocumento5 pagineGRDA Intro Bony PelvisKingNessuna valutazione finora
- Human Reflex Physiology: ExerciseDocumento4 pagineHuman Reflex Physiology: ExerciseGlainee esor selfroNessuna valutazione finora