Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Conners 3rd EditionDocumento11 pagineConners 3rd Editionapi-25939041967% (3)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Conners QuestionaireDocumento1 paginaConners QuestionaireSaiPremaVijayawadaNessuna valutazione finora
- DSM 5 - DSM 5Documento7 pagineDSM 5 - DSM 5Roxana ClsNessuna valutazione finora
- Achalasia: Department of MedicineDocumento21 pagineAchalasia: Department of Medicinekyliever100% (1)
- Usa Walnut Varieties 0Documento48 pagineUsa Walnut Varieties 0Oleg Tirsina100% (2)
- Hernia OSCE ExaminationDocumento3 pagineHernia OSCE ExaminationkylieverNessuna valutazione finora
- History:: Breast History and ExaminationDocumento4 pagineHistory:: Breast History and ExaminationkylieverNessuna valutazione finora
- An Overview of Cognitive Behavioral Therapy Webinar SlidesDocumento35 pagineAn Overview of Cognitive Behavioral Therapy Webinar Slideskyliever100% (1)
- OG 2.2 Anatomy of The Female Pelvis: Og 1.8 The Cardiotocograph Class Course Obstetrics and Gynaecology Code Title DateDocumento27 pagineOG 2.2 Anatomy of The Female Pelvis: Og 1.8 The Cardiotocograph Class Course Obstetrics and Gynaecology Code Title Datekyliever100% (2)
- Thyroid Gland OSCE ExaminationDocumento13 pagineThyroid Gland OSCE ExaminationkylieverNessuna valutazione finora
- ENT Emergency: James Paul O'NeillDocumento43 pagineENT Emergency: James Paul O'NeillkylieverNessuna valutazione finora
- OsteoarthritisDocumento40 pagineOsteoarthritiskylieverNessuna valutazione finora
- b2 s3 WritingDocumento8 pagineb2 s3 WritinglilalilakNessuna valutazione finora
- ENT EmergencyDocumento57 pagineENT EmergencykylieverNessuna valutazione finora
- First Grade Science Seasons LessonDocumento10 pagineFirst Grade Science Seasons Lessonapi-273149494100% (2)
- A Brief Legal History of Philippine EducationDocumento6 pagineA Brief Legal History of Philippine EducationZahjid CallangNessuna valutazione finora
- State and District Academic Standards Professional DevelopmentDocumento15 pagineState and District Academic Standards Professional Developmentapi-506887250Nessuna valutazione finora
- Thought Record Sheet AngerDocumento2 pagineThought Record Sheet AngerkylieverNessuna valutazione finora
- Psychopathy Checklist-Revised (PCL-R) : January 2016Documento5 paginePsychopathy Checklist-Revised (PCL-R) : January 2016kylieverNessuna valutazione finora
- Psychopathy Checklist: Screening Version (PCL:SV) : January 2016Documento5 paginePsychopathy Checklist: Screening Version (PCL:SV) : January 2016kylieverNessuna valutazione finora
- Wwa NodosumDocumento21 pagineWwa NodosumMu AbNessuna valutazione finora
- This Dysfunctional Thought Record Worksheet Is Divided Into 7 ColumnsDocumento2 pagineThis Dysfunctional Thought Record Worksheet Is Divided Into 7 ColumnskylieverNessuna valutazione finora
- Core Belief WorksheetDocumento1 paginaCore Belief WorksheetkylieverNessuna valutazione finora
- Pyoderma GangrenosumDocumento35 paginePyoderma GangrenosumkylieverNessuna valutazione finora
- AcromegalyDocumento2 pagineAcromegalykylieverNessuna valutazione finora
- Perinatal MedicineDocumento39 paginePerinatal MedicinekylieverNessuna valutazione finora
- PsychopathologyDocumento22 paginePsychopathologykylieverNessuna valutazione finora
- Diabetes Mellitus Type I DMI: Department of Family Medicine and General Practice RcsiDocumento25 pagineDiabetes Mellitus Type I DMI: Department of Family Medicine and General Practice RcsikylieverNessuna valutazione finora
- Maryam Fuad Ali - SC1 Obgyn: FibroidsDocumento1 paginaMaryam Fuad Ali - SC1 Obgyn: FibroidskylieverNessuna valutazione finora
- OG 1.3 - Preconception and Prenatal Care Jan 2015Documento19 pagineOG 1.3 - Preconception and Prenatal Care Jan 2015kylieverNessuna valutazione finora
- OG 1.4 - Normal Labour + Delivery - Jan 2015Documento20 pagineOG 1.4 - Normal Labour + Delivery - Jan 2015kylieverNessuna valutazione finora
- AutismDocumento3 pagineAutismkylieverNessuna valutazione finora
- Pediatric DermatologyDocumento10 paginePediatric DermatologykylieverNessuna valutazione finora
- Age Related Macular DegenerationDocumento26 pagineAge Related Macular DegenerationRebecca WongNessuna valutazione finora
- RecommendationDocumento1 paginaRecommendationAyush KumarNessuna valutazione finora
- Sosc1960 HkustDocumento4 pagineSosc1960 HkustMary LamNessuna valutazione finora
- V Turner Symbol Process SystemDocumento21 pagineV Turner Symbol Process SystemAlexandra Elizzabeth AndriesNessuna valutazione finora
- Future of Elearning in IndiaDocumento14 pagineFuture of Elearning in IndiaAnu Khurana ChawlaNessuna valutazione finora
- A Level Pure1 Oct2021 Mark SchemeDocumento27 pagineA Level Pure1 Oct2021 Mark Schememzino100406Nessuna valutazione finora
- Rebecca A. Endaya Beed-Iii Art Education: ExploreDocumento5 pagineRebecca A. Endaya Beed-Iii Art Education: ExploreBhecca Endaya0% (1)
- School Form 9 Report Card 2022Documento63 pagineSchool Form 9 Report Card 2022CYNTHIA CUSTODIONessuna valutazione finora
- Lipmans Thinking in Education PDFDocumento7 pagineLipmans Thinking in Education PDFLaura Nicoleta BorhanNessuna valutazione finora
- Sample of Form 4 English Daily Lesson Notes (For 21-25 Apr 2014)Documento3 pagineSample of Form 4 English Daily Lesson Notes (For 21-25 Apr 2014)globalventure557134100% (1)
- RA MASTERPLUMBING CDO July2018 PDFDocumento10 pagineRA MASTERPLUMBING CDO July2018 PDFPhilBoardResultsNessuna valutazione finora
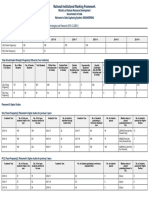
- Institute Name: Ambedkar Institute of Advanced Communication Technologies and Research (IR-E-C-32851)Documento7 pagineInstitute Name: Ambedkar Institute of Advanced Communication Technologies and Research (IR-E-C-32851)Ravi Ranjan KumarNessuna valutazione finora
- Wayne Visser: Speaker Biography Idea-Monger, Story-Teller, Meme-WeaverDocumento27 pagineWayne Visser: Speaker Biography Idea-Monger, Story-Teller, Meme-WeaverZola1348Nessuna valutazione finora
- PLC StrategiesDocumento3 paginePLC StrategiesGan Zi XiNessuna valutazione finora
- Madriaga, Rona Frances A.Documento6 pagineMadriaga, Rona Frances A.Jason L. Saldua,BSN,RNNessuna valutazione finora
- 2nd Periodical PerDevDocumento1 pagina2nd Periodical PerDevAbigail N. DitanNessuna valutazione finora
- EceDocumento67 pagineEceaditya_pundirNessuna valutazione finora
- 3 - Individual Differences Among LearnersDocumento8 pagine3 - Individual Differences Among LearnersDg HasmahNessuna valutazione finora
- Ciencias Sociales: Infinite Upware Soft S.A.SDocumento12 pagineCiencias Sociales: Infinite Upware Soft S.A.SSergio GarcíaNessuna valutazione finora
- Validacao Escala Espiritualidade Pinto - Pais RibeiroDocumento7 pagineValidacao Escala Espiritualidade Pinto - Pais RibeiroLucasFelipeRibeiroNessuna valutazione finora
- College of New Caledonia Application FormDocumento2 pagineCollege of New Caledonia Application Formdaljit8199Nessuna valutazione finora
- Abrams - Peirce, Kant, and Apel On Transcendental Semiotics. The Unity of Apperception and The Deduction of The Categories of SignsDocumento52 pagineAbrams - Peirce, Kant, and Apel On Transcendental Semiotics. The Unity of Apperception and The Deduction of The Categories of Signskafirun100% (1)
- Detailed Lesson Plan For Submission No 4Documento5 pagineDetailed Lesson Plan For Submission No 4Tromar Castillo LorestoNessuna valutazione finora
- Digital Footprint AssignmentDocumento2 pagineDigital Footprint AssignmentPAING LIN HTIKENessuna valutazione finora
- Basic National Education - Report of The Zakir Husain CommitteeDocumento205 pagineBasic National Education - Report of The Zakir Husain CommitteeMehwash DilshadNessuna valutazione finora
- Nwineh, L.1 & Okwelle, P.C.2 1Documento11 pagineNwineh, L.1 & Okwelle, P.C.2 1paul okwelleNessuna valutazione finora