Potrebbero piacerti anche
- Anovulation, Delayed Ovulation and Luteal InsufficiencyDocumento4 pagineAnovulation, Delayed Ovulation and Luteal InsufficiencySanjay C. Parmar0% (1)
- Mayan Abdominal Massage For TTC-Easy Self Fertility Massage That Helped Me Get Pregnant!Documento9 pagineMayan Abdominal Massage For TTC-Easy Self Fertility Massage That Helped Me Get Pregnant!miruna_macaveiNessuna valutazione finora
- 3-Step Cycle Syncing GuideDocumento13 pagine3-Step Cycle Syncing Guidehuracanrojo94100% (2)
- Is Soy Bad For PcosDocumento13 pagineIs Soy Bad For PcosJudi Ann MagsacayNessuna valutazione finora
- Mothers Circle: The Birth of Your Sacred VillageDa EverandMothers Circle: The Birth of Your Sacred VillageNessuna valutazione finora
- WOLFPACK YOGA - Private Session Intake FormDocumento2 pagineWOLFPACK YOGA - Private Session Intake Formnatalie burtneyNessuna valutazione finora
- Bellymap Parent HandoutDocumento2 pagineBellymap Parent HandoutChristine Duclos ImlerNessuna valutazione finora
- Pregnancy Made Confortable With Yoga & Dietetics: Yogic exercises & nutrition to make motherhood easyDa EverandPregnancy Made Confortable With Yoga & Dietetics: Yogic exercises & nutrition to make motherhood easyNessuna valutazione finora
- Herbs 4 Kids RommDocumento31 pagineHerbs 4 Kids RommMariaNessuna valutazione finora
- The Rhythms of Wellness: Follow the wisdom of the ancient sages and align with Nature's cycles for greater health and wellbeing.Da EverandThe Rhythms of Wellness: Follow the wisdom of the ancient sages and align with Nature's cycles for greater health and wellbeing.Nessuna valutazione finora
- Quick Guide To Charting Your Cycle: Giuliana Serena's With A Moon Phase CalendarDocumento1 paginaQuick Guide To Charting Your Cycle: Giuliana Serena's With A Moon Phase CalendarAlbertGyörgynéFeketeJuditNessuna valutazione finora
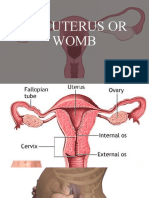
- The Uterus or WombDocumento38 pagineThe Uterus or WombmuwahNessuna valutazione finora
- Cycle SyncingDocumento43 pagineCycle SyncingHeShot MeDownNessuna valutazione finora
- Foods For FertilityDocumento2 pagineFoods For FertilityKaye HeyesNessuna valutazione finora
- Vibrant Blue Oils Recipes For ResilienceDocumento67 pagineVibrant Blue Oils Recipes For ResilienceSofia BouçadasNessuna valutazione finora
- Fertility YogaDocumento6 pagineFertility Yoganikjadhav100% (2)
- Maya Abominal MassageDocumento1 paginaMaya Abominal MassageMaureenManningNessuna valutazione finora
- Latent Phase of LabourDocumento10 pagineLatent Phase of LabourFELIX CLINENessuna valutazione finora
- Pure Nurture: A Holistic Guide to a Healthy BabyDa EverandPure Nurture: A Holistic Guide to a Healthy BabyNessuna valutazione finora
- Asana For Relieving PMSDocumento4 pagineAsana For Relieving PMSgurunathnkulkarniNessuna valutazione finora
- Lunar Chart GuideDocumento9 pagineLunar Chart GuideElena M100% (1)
- The Menstrual Cycle WorksheetDocumento2 pagineThe Menstrual Cycle Worksheetapi-383924075% (4)
- Pregnancy, Birth and Beyond: A Spiritual and Practical GuideDa EverandPregnancy, Birth and Beyond: A Spiritual and Practical GuideNessuna valutazione finora
- MEDITATION MAGNIFY YOUR RADIANCE Lion's Paws With Breath of FireDocumento2 pagineMEDITATION MAGNIFY YOUR RADIANCE Lion's Paws With Breath of FireNicole HawkinsNessuna valutazione finora
- Pelvic Liberation: Using Yoga, Self-Inquiry, and Breath Awareness for Pelvic HealthDa EverandPelvic Liberation: Using Yoga, Self-Inquiry, and Breath Awareness for Pelvic HealthValutazione: 5 su 5 stelle5/5 (1)
- Wellness Wisdom: 31 Ways to Nourish Your Mind, Body, & SpiritDa EverandWellness Wisdom: 31 Ways to Nourish Your Mind, Body, & SpiritNessuna valutazione finora
- Painless Childbirth: An All-Natural Nutrition PlanDa EverandPainless Childbirth: An All-Natural Nutrition PlanNessuna valutazione finora
- Embrace Your Elegant Power: Your Path to Success Through EaseDa EverandEmbrace Your Elegant Power: Your Path to Success Through EaseNessuna valutazione finora
- Pregnancy Brain: A Mind-Body Approach To Stress Management During A High-Risk Pregnancy - GeneralDocumento5 paginePregnancy Brain: A Mind-Body Approach To Stress Management During A High-Risk Pregnancy - GeneralcolomehuNessuna valutazione finora
- Pelvic Girdle Pain (PGP) : A Guide For You and Your RelativesDocumento8 paginePelvic Girdle Pain (PGP) : A Guide For You and Your RelativesrahmawatusNessuna valutazione finora
- Intro To The 6 Tissue States Herbalism CourseDocumento3 pagineIntro To The 6 Tissue States Herbalism CourseAlejandra GuerreroNessuna valutazione finora
- Stronger: The honest guide to healing and rebuilding after pregnancy and birthDa EverandStronger: The honest guide to healing and rebuilding after pregnancy and birthNessuna valutazione finora
- Holistic Pregnancy Manual: Maternal Health Manuals, #1Da EverandHolistic Pregnancy Manual: Maternal Health Manuals, #1Nessuna valutazione finora
- Pelvic Pain Game Changer: 6 Steps to a Healthier YouDa EverandPelvic Pain Game Changer: 6 Steps to a Healthier YouNessuna valutazione finora
- Boost Getting Pregnant: Surprisingly Simple Natural Ways To Remedy InfertilityDa EverandBoost Getting Pregnant: Surprisingly Simple Natural Ways To Remedy InfertilityNessuna valutazione finora
- 50 Affirmations For A Fertile Mind, Heart & SoulDocumento104 pagine50 Affirmations For A Fertile Mind, Heart & SoulKarishma SethNessuna valutazione finora
- When Women Gather: A Guidebook for Hosting Gatherings for WomenDa EverandWhen Women Gather: A Guidebook for Hosting Gatherings for WomenNessuna valutazione finora
- Consensus On Current Management of EndometriosisDocumento17 pagineConsensus On Current Management of EndometriosisCristina BravoNessuna valutazione finora
- Seed Rotation Ebook Final 2Documento10 pagineSeed Rotation Ebook Final 2Andreea Cretiu100% (3)
- 8 Prenatal ExercisesDocumento12 pagine8 Prenatal ExercisesJeane Rose PurazoNessuna valutazione finora
- Hardwired for Love: Nurturing Yourself to Vibrant HealthDa EverandHardwired for Love: Nurturing Yourself to Vibrant HealthNessuna valutazione finora
- Birth AffirmationsDocumento4 pagineBirth AffirmationsPaula Cohen SchlemmerNessuna valutazione finora
- Baby SuppliesDocumento124 pagineBaby SuppliesWell-Being per diemNessuna valutazione finora
- Fix Your Period Cleanse Prep PDFDocumento4 pagineFix Your Period Cleanse Prep PDFblizzNessuna valutazione finora
- Pelvic Girdle Pain LeafletDocumento5 paginePelvic Girdle Pain LeafletagniosaiNessuna valutazione finora
- ' Yoga Vidhya ': The Art & Science of SadayurarogyaDocumento10 pagine' Yoga Vidhya ': The Art & Science of SadayurarogyaAnjali KandarpaNessuna valutazione finora
- Circles of Healing: The Complete Guide to Healing With Massage & YogaDa EverandCircles of Healing: The Complete Guide to Healing With Massage & YogaNessuna valutazione finora
- Holistic Postpartum Manual: Maternal Health Manuals, #3Da EverandHolistic Postpartum Manual: Maternal Health Manuals, #3Nessuna valutazione finora
- FPQC Positions For LaborDocumento3 pagineFPQC Positions For LaborAukia HyuugaNessuna valutazione finora
- Woman: An Historical Gynæcological and Anthropological CompendiumDa EverandWoman: An Historical Gynæcological and Anthropological CompendiumNessuna valutazione finora
- Liquichek Elevated CRP Control Levels 1, 2 and 3: Revision Date 2022-05-26 Indicates Revised InformationDocumento1 paginaLiquichek Elevated CRP Control Levels 1, 2 and 3: Revision Date 2022-05-26 Indicates Revised InformationowoladeidowuNessuna valutazione finora
- AGILENT GeneExpression Two Color v6.5Documento92 pagineAGILENT GeneExpression Two Color v6.5Anonymous PsEz5kGVaeNessuna valutazione finora
- Student Exploration: Evolution: Mutation and Selection Gizmo AnswersDocumento8 pagineStudent Exploration: Evolution: Mutation and Selection Gizmo Answersthanossssss57% (7)
- SCP Production NotesDocumento4 pagineSCP Production Notessaurabh pandeyNessuna valutazione finora
- Candida Albicans (ATCC: Product SheetDocumento2 pagineCandida Albicans (ATCC: Product SheetTuan TranNessuna valutazione finora
- Beic Listado Completo 2012 1Documento137 pagineBeic Listado Completo 2012 1lolita3077Nessuna valutazione finora
- Biofertilizer For Crop Production and Soil Fertility: August 2018Documento9 pagineBiofertilizer For Crop Production and Soil Fertility: August 2018GnanakumarNessuna valutazione finora
- Department of Molecular Virology: COVID-19 (Corona) VirusDocumento1 paginaDepartment of Molecular Virology: COVID-19 (Corona) VirusHabib ur-RehmanNessuna valutazione finora
- Supplement Black BookDocumento33 pagineSupplement Black Booktweetybyrd443013Nessuna valutazione finora
- Evidence For Evolution Guided Inquiry WorksheetDocumento6 pagineEvidence For Evolution Guided Inquiry WorksheetMya IrelandNessuna valutazione finora
- Vitamin C Ascorbic AcidDocumento21 pagineVitamin C Ascorbic Acidapi-388948078Nessuna valutazione finora
- Bio Test Gym 2a 2quarter 2022 BDocumento10 pagineBio Test Gym 2a 2quarter 2022 BJohny CashNessuna valutazione finora
- The Origin of Eukaryotes: A ReappraisalDocumento9 pagineThe Origin of Eukaryotes: A Reappraisalkirowasi94Nessuna valutazione finora
- Passive and Active Transport Internet AssignmentDocumento4 paginePassive and Active Transport Internet AssignmentShalu PundirNessuna valutazione finora
- AnthropologyDocumento209 pagineAnthropologyStiff Yilma50% (2)
- Forensics 12-13 TestDocumento3 pagineForensics 12-13 Testmemmy3697Nessuna valutazione finora
- Fifth Edition Answers To End-Of-Chapter Questions: GCSE Biology For YouDocumento1 paginaFifth Edition Answers To End-Of-Chapter Questions: GCSE Biology For YouclydeNessuna valutazione finora
- Discuss Genetic Factors in AggressionDocumento2 pagineDiscuss Genetic Factors in AggressionmopheadfattyNessuna valutazione finora
- Systematic Anatomy OF Dicqtyledons: Ajay Book ServiceDocumento543 pagineSystematic Anatomy OF Dicqtyledons: Ajay Book ServiceJOSE FRANCISCO FRANCO NAVIANessuna valutazione finora
- Ijms 22 04779Documento15 pagineIjms 22 04779Sofiya -Nessuna valutazione finora
- Biotic Stree and Yield LossDocumento258 pagineBiotic Stree and Yield LossDhanraj KumarNessuna valutazione finora
- CYPERMETHRINDocumento7 pagineCYPERMETHRINJurgen SchirmacherNessuna valutazione finora
- Environmental Case Study of Water Quality and Climate Change Resulting A Mass Mortality of Fish at Taj Boudi of BijapurDocumento7 pagineEnvironmental Case Study of Water Quality and Climate Change Resulting A Mass Mortality of Fish at Taj Boudi of BijapurIOSRjournalNessuna valutazione finora
- Kitar KrebsDocumento5 pagineKitar KrebsAlfonso RobertNessuna valutazione finora
- Blotting TechniquesDocumento31 pagineBlotting TechniquesRahul Amin Sheikh 19MSM0114Nessuna valutazione finora
- Integumentary Sensory Organs in CrocodiliansDocumento10 pagineIntegumentary Sensory Organs in CrocodiliansEduardo LeónNessuna valutazione finora
- Prefixes, Suffixes, Roots PDFDocumento37 paginePrefixes, Suffixes, Roots PDFVu SangNessuna valutazione finora
- Biotechnology For SustainabilityDocumento552 pagineBiotechnology For SustainabilitySubhash Janardhan Bhore, PhD100% (1)
- About MangrovesDocumento5 pagineAbout MangrovesKathleen Laum CabanlitNessuna valutazione finora