Potrebbero piacerti anche
- BORB Birmingham Object Recognition BatteryDocumento5 pagineBORB Birmingham Object Recognition BatteryAnaaaerobios0% (1)
- Prochaska - Transtheoretical PDFDocumento13 pagineProchaska - Transtheoretical PDFMaria Cecilia Oñederra LlanosNessuna valutazione finora
- Integrative ApproachesDocumento28 pagineIntegrative ApproachespsicandreiaNessuna valutazione finora
- Integrative Psychotherapy PDFDocumento27 pagineIntegrative Psychotherapy PDFdev0% (1)
- The Generalizability of The Psychoanalytic Concept of The Working Alliance - E Bordin 1979Documento9 pagineThe Generalizability of The Psychoanalytic Concept of The Working Alliance - E Bordin 1979Manuel Pernetas100% (3)
- Eclectic and Integrative Approaches To CounsellingDocumento18 pagineEclectic and Integrative Approaches To CounsellingAlbert Muya Muraya100% (1)
- APA 7th Edition LLC 2020Documento10 pagineAPA 7th Edition LLC 2020Juliana Giraldo Rivera100% (3)
- Multi-Criteria Decision MakingDocumento52 pagineMulti-Criteria Decision MakingD'Mhan Mbozo100% (1)
- Horvath Et Al (2011) Alliance I 20736Documento8 pagineHorvath Et Al (2011) Alliance I 20736Marwa ElsheikhNessuna valutazione finora
- Relaçao Terapeutica, HorvathDocumento6 pagineRelaçao Terapeutica, HorvathÂngela FerreiraNessuna valutazione finora
- Revisiting Bordin's Theory On The Therapeutic Alliance: Implications For Family TherapyDocumento14 pagineRevisiting Bordin's Theory On The Therapeutic Alliance: Implications For Family TherapyJomar BumidangNessuna valutazione finora
- HorvathDocumento14 pagineHorvathFlorencia FerreiraNessuna valutazione finora
- Therapeutic Alliance HorvathDocumento14 pagineTherapeutic Alliance HorvathGloria KentNessuna valutazione finora
- World Psychiatry - 2023 - Wampold - The Alliance in Mental Health Care Conceptualization Evidence and ClinicalDocumento17 pagineWorld Psychiatry - 2023 - Wampold - The Alliance in Mental Health Care Conceptualization Evidence and Clinicalekaterinavalerieva91Nessuna valutazione finora
- Wampold, B. 2015. How Important Are The Common Factors in Psychotherapy. An UpdateDocumento8 pagineWampold, B. 2015. How Important Are The Common Factors in Psychotherapy. An UpdateMARIO APPELIUS SANHUEZANessuna valutazione finora
- Alliance in Couple and Family TherapyDocumento9 pagineAlliance in Couple and Family TherapyQuisocNessuna valutazione finora
- Generic ModelDocumento21 pagineGeneric ModelDario CornejoNessuna valutazione finora
- Therapeutic CommanalitiesDocumento8 pagineTherapeutic CommanalitiesRoshni TripathyNessuna valutazione finora
- Adam O Horvath Alliance in PychoterapyDocumento15 pagineAdam O Horvath Alliance in PychoterapyArmando Alexander NapoletanoNessuna valutazione finora
- Orlinsky GenericModelAfter25Yrs2009Documento22 pagineOrlinsky GenericModelAfter25Yrs2009Cesar BermudezNessuna valutazione finora
- Therapist Interpretation, Patient-Therapist Interpersonal Process, and Outcome in Psychodynamic Psychotherapy For Avoidant Personality DisorderDocumento18 pagineTherapist Interpretation, Patient-Therapist Interpersonal Process, and Outcome in Psychodynamic Psychotherapy For Avoidant Personality DisorderPamela Cortés PeñaNessuna valutazione finora
- The Search For Common Factors in PsychotDocumento20 pagineThe Search For Common Factors in PsychotYoshita AgarwalNessuna valutazione finora
- The Therapeutic Alliance in Couples and Family TherapyDocumento10 pagineThe Therapeutic Alliance in Couples and Family TherapySophiez0257Nessuna valutazione finora
- Estructura Factores ComunesDocumento13 pagineEstructura Factores ComunesCesar BermudezNessuna valutazione finora
- Experiencing Psychotherapy Grounded TheoryDocumento28 pagineExperiencing Psychotherapy Grounded Theorypsicandreia100% (1)
- 2017 Book InternationalPerspectivesOnPsy PDFDocumento273 pagine2017 Book InternationalPerspectivesOnPsy PDFAna Alice Reis Pieretti100% (1)
- Therapist Self-Disclosure and Immediacy - A Qualitative Meta-AnalyDocumento30 pagineTherapist Self-Disclosure and Immediacy - A Qualitative Meta-AnalyHarsiddhi ThakralNessuna valutazione finora
- Alliance in Couple and Family TherapyDocumento10 pagineAlliance in Couple and Family TherapylpandradevNessuna valutazione finora
- Herbert y Gaudiano (2013) : The Importance of Theory in Cognitive Behavior Therapy: A Perspective of Contextual Behavioral ScienceDocumento12 pagineHerbert y Gaudiano (2013) : The Importance of Theory in Cognitive Behavior Therapy: A Perspective of Contextual Behavioral SciencePablo Valencia MeléndezNessuna valutazione finora
- Towards A Relationally-Orientated Approach To Therapy - Empirical Support and AnalysisDocumento18 pagineTowards A Relationally-Orientated Approach To Therapy - Empirical Support and AnalysisJames BarnesNessuna valutazione finora
- Common Factors + DefinitionDocumento8 pagineCommon Factors + DefinitionVal AvivNessuna valutazione finora
- Therapist Self-Disclosure: Research-Based Suggestions For PractitionersDocumento11 pagineTherapist Self-Disclosure: Research-Based Suggestions For PractitionerslizleeasNessuna valutazione finora
- Mycroanalysis in Communication PsychotherapyDocumento20 pagineMycroanalysis in Communication PsychotherapyEvelyn PeckelNessuna valutazione finora
- Orlinsky - The Generic Model of PsychotherapyDocumento22 pagineOrlinsky - The Generic Model of PsychotherapyIgnacia HuckeNessuna valutazione finora
- 25 Years of Systemic Therapies Research Progress and PromiseDocumento18 pagine25 Years of Systemic Therapies Research Progress and Promisesergioem40100% (1)
- Relational Aspects of Intersubjectivity Therapy and Gestalt TheraDocumento59 pagineRelational Aspects of Intersubjectivity Therapy and Gestalt Therascottpetrie67% (3)
- Empathy and Client OutcomeDocumento26 pagineEmpathy and Client OutcomeGloria KentNessuna valutazione finora
- Beck, Meichenbaum, and Strupp - Models ComparisonDocumento11 pagineBeck, Meichenbaum, and Strupp - Models ComparisonEdgarAlexandreNessuna valutazione finora
- Psychoanalytic Therapy. Principles and Application (Franz Alexander) (Z-Library)Documento367 paginePsychoanalytic Therapy. Principles and Application (Franz Alexander) (Z-Library)Ann TrầnNessuna valutazione finora
- Gabbard The Effect of Therapist Interventions On The Therapeutic Alliance With Borderline PatientsDocumento31 pagineGabbard The Effect of Therapist Interventions On The Therapeutic Alliance With Borderline PatientsPepe Serrano RodríguezNessuna valutazione finora
- Collusion Revisited: A Narrative Review of Dyadic CollusionsDocumento9 pagineCollusion Revisited: A Narrative Review of Dyadic Collusionssanskarbarekar789Nessuna valutazione finora
- How Important Are The Common Factors in Psychotherapy? An UpdateDocumento8 pagineHow Important Are The Common Factors in Psychotherapy? An UpdateCoordinacionPsicologiaVizcayaGuaymasNessuna valutazione finora
- Wampold, 2015 - How - Important - Are - The - Common - FactorsDocumento6 pagineWampold, 2015 - How - Important - Are - The - Common - Factorsup201900768Nessuna valutazione finora
- Attachment Disturbances in Adults Treatment For Comprehensive RepairDocumento5 pagineAttachment Disturbances in Adults Treatment For Comprehensive RepairPavel BalanNessuna valutazione finora
- Parish Eagle Attachment 2003Documento16 pagineParish Eagle Attachment 2003inetwork2001100% (1)
- Gold FriedDocumento10 pagineGold FriedPamela Cortés PeñaNessuna valutazione finora
- WHATISPATHOLOGYDocumento33 pagineWHATISPATHOLOGYtabinanadeemNessuna valutazione finora
- Handbook of Psychotherapy Integration Cap 1Documento43 pagineHandbook of Psychotherapy Integration Cap 1Vanessa Granada JiménezNessuna valutazione finora
- Psychotherapy Integration Via Theoretical Unification: Warren W. TryonDocumento26 paginePsychotherapy Integration Via Theoretical Unification: Warren W. Tryonmelpomena81Nessuna valutazione finora
- Gazzola Stalikas 2004Documento22 pagineGazzola Stalikas 2004Jules IuliaNessuna valutazione finora
- The 'Generic Model of Psychotherapy' After 25 Years (Orlynsky) PDFDocumento21 pagineThe 'Generic Model of Psychotherapy' After 25 Years (Orlynsky) PDFJoaquin OlivaresNessuna valutazione finora
- Systemic Family Therapy Competences in Child and Adolescent Mental Health CareDocumento18 pagineSystemic Family Therapy Competences in Child and Adolescent Mental Health Careselmaozdemir1907Nessuna valutazione finora
- DeconstructingtheAlliance KrauseAltimirHorvath 2011 Published VersionDocumento18 pagineDeconstructingtheAlliance KrauseAltimirHorvath 2011 Published VersionMario VillegasNessuna valutazione finora
- The Role of Relationship and Technique in Therapeutic ChangeDocumento10 pagineThe Role of Relationship and Technique in Therapeutic ChangePamela Cortés PeñaNessuna valutazione finora
- Escudero 2016 Journal of Family TherapyDocumento5 pagineEscudero 2016 Journal of Family TherapyManuel Antonio Sandoval JiménezNessuna valutazione finora
- Psychotherapy Research: Please Scroll Down For ArticleDocumento15 paginePsychotherapy Research: Please Scroll Down For ArticleJoana Maestra CuturaNessuna valutazione finora
- Content ServerDocumento7 pagineContent ServerAna Rita SerraNessuna valutazione finora
- Congruenceand Therapeutic PresenceDocumento20 pagineCongruenceand Therapeutic PresenceNadir KhanNessuna valutazione finora
- Becoming A Postmodern TherapistDocumento31 pagineBecoming A Postmodern TherapistManuel Enrique Huertas RomanNessuna valutazione finora
- Principles of Intensive PsychotherapyDa EverandPrinciples of Intensive PsychotherapyValutazione: 4.5 su 5 stelle4.5/5 (3)
- What Psychotherapists Learn from Their ClientsDa EverandWhat Psychotherapists Learn from Their ClientsNessuna valutazione finora
- Somatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesDa EverandSomatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesChristos CharisNessuna valutazione finora
- Epidemiología Psiquiátrica en ArgentinaDocumento10 pagineEpidemiología Psiquiátrica en ArgentinaAnaaaerobiosNessuna valutazione finora
- Aportes y Limitaciones Del Boston Naming Test: Evidencia A Partir de Controles ColombianosDocumento8 pagineAportes y Limitaciones Del Boston Naming Test: Evidencia A Partir de Controles ColombianosAnaaaerobiosNessuna valutazione finora
- Decision-Making Steps Tools For A Nonviolence PDFDocumento1 paginaDecision-Making Steps Tools For A Nonviolence PDFAnaaaerobiosNessuna valutazione finora
- Central and Peripheral Components of Working Memory StorageDocumento1 paginaCentral and Peripheral Components of Working Memory StorageAnaaaerobiosNessuna valutazione finora
- "Five Digit Test": Minilexical Measurement of Mental Mechanics Cognitive Reactions and DecisionsDocumento1 pagina"Five Digit Test": Minilexical Measurement of Mental Mechanics Cognitive Reactions and DecisionsAnaaaerobiosNessuna valutazione finora
- BDNFDocumento14 pagineBDNFAnaaaerobiosNessuna valutazione finora
- Epidemiología de La Salud Mental en ArgentinaDocumento9 pagineEpidemiología de La Salud Mental en ArgentinaAnaaaerobiosNessuna valutazione finora
- Can Infection Lead To Mental IllnessDocumento87 pagineCan Infection Lead To Mental IllnessAnaaaerobiosNessuna valutazione finora
- Beta Amiloide y Sueño Diurno Excesivo Carvalho 2018Documento9 pagineBeta Amiloide y Sueño Diurno Excesivo Carvalho 2018AnaaaerobiosNessuna valutazione finora
- Reproducción VisualDocumento6 pagineReproducción VisualAnaaaerobiosNessuna valutazione finora
- Adultos Sanos VariabilityDocumento16 pagineAdultos Sanos VariabilityAnaaaerobiosNessuna valutazione finora
- Reproducción VisualDocumento6 pagineReproducción VisualAnaaaerobiosNessuna valutazione finora
- EP-1992-Cx DX Bank of BrainDocumento4 pagineEP-1992-Cx DX Bank of BrainAnaaaerobiosNessuna valutazione finora
- 2017-Soledad y Carga Amiloide en Corteza Cerebral - Donovan2016Documento8 pagine2017-Soledad y Carga Amiloide en Corteza Cerebral - Donovan2016AnaaaerobiosNessuna valutazione finora
- Atributos Visuales y No Visuales en El Reconocimiento Visual de ObjetosDocumento8 pagineAtributos Visuales y No Visuales en El Reconocimiento Visual de ObjetosAnaaaerobiosNessuna valutazione finora
- Aportes y Limitaciones Del Boston Naming Test: Evidencia A Partir de Controles ColombianosDocumento8 pagineAportes y Limitaciones Del Boston Naming Test: Evidencia A Partir de Controles ColombianosAnaaaerobiosNessuna valutazione finora
- 2017-Soledad y Carga Amiloide en Corteza Cerebral - Donovan2016 PDFDocumento8 pagine2017-Soledad y Carga Amiloide en Corteza Cerebral - Donovan2016 PDFAnaaaerobiosNessuna valutazione finora
- Simons On WritingDocumento8 pagineSimons On WritingramyresdavidNessuna valutazione finora
- BDNFDocumento14 pagineBDNFAnaaaerobiosNessuna valutazione finora
- A Decade of Contributions To Understanding and Ameliorating Attention Deficit-Hyperactivity DisorderDocumento4 pagineA Decade of Contributions To Understanding and Ameliorating Attention Deficit-Hyperactivity DisorderAnaaaerobiosNessuna valutazione finora
- Memoria de TrabajoDocumento15 pagineMemoria de TrabajoAnaaaerobiosNessuna valutazione finora
- Cancelacion DVT (6y9)Documento6 pagineCancelacion DVT (6y9)AnaaaerobiosNessuna valutazione finora
- SDMT QsDocumento6 pagineSDMT QsAnaaaerobios100% (1)
- Cognitive Impairment in Coeliac Disease Improves On A Gluten-Free Diet and Correlates With Histological and Serological Indices of Disease SeverityDocumento11 pagineCognitive Impairment in Coeliac Disease Improves On A Gluten-Free Diet and Correlates With Histological and Serological Indices of Disease SeverityAnaaaerobiosNessuna valutazione finora
- Beta Amiloide 42Documento7 pagineBeta Amiloide 42AnaaaerobiosNessuna valutazione finora
- 2016 Boston ColombiaDocumento8 pagine2016 Boston ColombiaAnaaaerobiosNessuna valutazione finora
- A Decade of Contributions To Understanding and Ameliorating Attention Deficit-Hyperactivity DisorderDocumento4 pagineA Decade of Contributions To Understanding and Ameliorating Attention Deficit-Hyperactivity DisorderAnaaaerobiosNessuna valutazione finora
- BDNFDocumento14 pagineBDNFAnaaaerobiosNessuna valutazione finora
- Guía de Buena Práctica para El Diagnóstico de Los Trastornos Del Espectro AutistaDocumento12 pagineGuía de Buena Práctica para El Diagnóstico de Los Trastornos Del Espectro AutistaEquipo de Orientación Liceo CastillaNessuna valutazione finora
- Quantum Mechanics A Paradigms Approach 1st Edition Mcintyre Solutions ManualDocumento36 pagineQuantum Mechanics A Paradigms Approach 1st Edition Mcintyre Solutions ManualMicheleWallsertso100% (16)
- The Soldier's Tale Programme NotesDocumento6 pagineThe Soldier's Tale Programme NotesStefano BoccacciNessuna valutazione finora
- DLL - Math 2 - Q1 - W1Documento10 pagineDLL - Math 2 - Q1 - W1Jo HannaNessuna valutazione finora
- Capstone Project ProposDocumento10 pagineCapstone Project Proposapi-631009395Nessuna valutazione finora
- WK10 Lesson PDFDocumento5 pagineWK10 Lesson PDFPaul macaraegNessuna valutazione finora
- Digital Booklet - X (Deluxe Version) - UnlockedDocumento10 pagineDigital Booklet - X (Deluxe Version) - UnlockedНики ДимитровNessuna valutazione finora
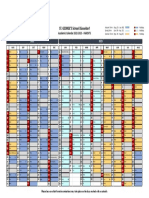
- Academic Calendar 22-23 - SGSD - PARENTS - FINALDocumento1 paginaAcademic Calendar 22-23 - SGSD - PARENTS - FINALfloraNessuna valutazione finora
- Personal Information: Algeria / Master'S Degree 2018989299 / 22DZ011511Documento6 paginePersonal Information: Algeria / Master'S Degree 2018989299 / 22DZ011511Mira GouffiNessuna valutazione finora
- Posse ProcessDocumento4 paginePosse Processapi-597185067Nessuna valutazione finora
- PhonicsDocumento47 paginePhonicskhairul5115100% (1)
- Teaching Methods in ScienceDocumento4 pagineTeaching Methods in ScienceJavy mae masbateNessuna valutazione finora
- Naturalistic Developmental Behavioral Interventions Empirically Validated Treatments For Autism Spectrum DisorderDocumento18 pagineNaturalistic Developmental Behavioral Interventions Empirically Validated Treatments For Autism Spectrum DisorderLuis SeixasNessuna valutazione finora
- AurangabadDocumento3 pagineAurangabadRamdas NagareNessuna valutazione finora
- Ncrasem PDFDocumento195 pagineNcrasem PDFKumar Goud.KNessuna valutazione finora
- If Clauses IIDocumento4 pagineIf Clauses IICarolina Leiva PalmaNessuna valutazione finora
- Foster Ezell ResumeDocumento1 paginaFoster Ezell Resumeapi-448653878Nessuna valutazione finora
- PDF Q1 Mod 1 EIM GRADE 12 NewDocumento10 paginePDF Q1 Mod 1 EIM GRADE 12 NewCloud DullasNessuna valutazione finora
- Why Emotional Literacy Is Good For Your SchoolDocumento14 pagineWhy Emotional Literacy Is Good For Your SchoolBesjana KoçiNessuna valutazione finora
- 10 Tools To Make A Bootable USB From An ISO FileDocumento10 pagine10 Tools To Make A Bootable USB From An ISO Filedds70Nessuna valutazione finora
- Procrastination: Reasons Why People ProcrastinateDocumento8 pagineProcrastination: Reasons Why People Procrastinatehuzaifa anwarNessuna valutazione finora
- LO170 - 46C - 003basicsDocumento28 pagineLO170 - 46C - 003basicsmkumarshahiNessuna valutazione finora
- Akhlaq Model - Al Ghazali DiscourseDocumento8 pagineAkhlaq Model - Al Ghazali DiscourseshizaranaNessuna valutazione finora
- Effectiveness of Talent Management at BRACDocumento40 pagineEffectiveness of Talent Management at BRACM.N.G Al FirojNessuna valutazione finora
- A Co. S10 PT PlanDocumento3 pagineA Co. S10 PT PlancorinjoelNessuna valutazione finora
- Essaynumber 4Documento3 pagineEssaynumber 4api-285330955Nessuna valutazione finora
- Literary CriticismDocumento4 pagineLiterary CriticismMadeleine BorromeoNessuna valutazione finora
- TABLE OF CONTENTS FINAL - 2ndDocumento10 pagineTABLE OF CONTENTS FINAL - 2ndKaren CobachaNessuna valutazione finora
- Hydrophobia ProjectDocumento4 pagineHydrophobia ProjectAnonymous GamerNessuna valutazione finora