Potrebbero piacerti anche
- Individualized Education PlanDocumento7 pagineIndividualized Education PlanElaine Aninang Hupeda100% (2)
- Checklist: Mobile Crane SafetyDocumento2 pagineChecklist: Mobile Crane SafetyJohn Kurong100% (5)
- ANP Heart Anatomy & PhysiologyDocumento3 pagineANP Heart Anatomy & PhysiologySheana Tmpl100% (1)
- MKSAP NotesDocumento31 pagineMKSAP NotesJared MasonNessuna valutazione finora
- Presentation On Myasthenia Gravis: Presented By: Sandhya Harbola M.Sc. Nursing 1 Year PcnmsDocumento32 paginePresentation On Myasthenia Gravis: Presented By: Sandhya Harbola M.Sc. Nursing 1 Year PcnmsShubham Singh Bisht100% (3)
- Fast Facts: Recognizing Refractory Myasthenia GravisDa EverandFast Facts: Recognizing Refractory Myasthenia GravisNessuna valutazione finora
- Choledocholithias PathophysiologyDocumento2 pagineCholedocholithias PathophysiologySheana Tmpl100% (2)
- Choledocholithias PathophysiologyDocumento2 pagineCholedocholithias PathophysiologySheana Tmpl100% (2)
- Piaggio MP3 300 Ibrido LT MY 2010 (En)Documento412 paginePiaggio MP3 300 Ibrido LT MY 2010 (En)Manualles100% (3)
- Pathophysiology of Coronary Artery Disease and Myocardial InfarctionDocumento2 paginePathophysiology of Coronary Artery Disease and Myocardial InfarctionSheana TmplNessuna valutazione finora
- MS 1 PERIOPERATIVE NURSING ROLES AND RESPONSIBILITIESDocumento41 pagineMS 1 PERIOPERATIVE NURSING ROLES AND RESPONSIBILITIESSheana TmplNessuna valutazione finora
- Terminal Tractors and Trailers 6.1Documento7 pagineTerminal Tractors and Trailers 6.1lephuongdongNessuna valutazione finora
- Presentation On Data Integrity in PharmaDocumento80 paginePresentation On Data Integrity in Pharmaskvemula67% (3)
- Diploma Pharmacy First Year - Hap - MCQSDocumento13 pagineDiploma Pharmacy First Year - Hap - MCQSAnitha Mary Dambale91% (33)
- Community Health Nursing Practice Questions With RationalesDocumento15 pagineCommunity Health Nursing Practice Questions With RationalesFelice Lamzon Labrador100% (2)
- Community Health Nursing Practice Questions With RationalesDocumento15 pagineCommunity Health Nursing Practice Questions With RationalesFelice Lamzon Labrador100% (2)
- The Turbo Air 6000 Centrifugal Compressor Handbook AAEDR-H-082 Rev 05 TA6000Documento137 pagineThe Turbo Air 6000 Centrifugal Compressor Handbook AAEDR-H-082 Rev 05 TA6000Rifki TriAditiya PutraNessuna valutazione finora
- D Formation Damage StimCADE FDADocumento30 pagineD Formation Damage StimCADE FDAEmmanuel EkwohNessuna valutazione finora
- Lambert-Eaton Myasthenic Syndrome Dr. SitoyDocumento4 pagineLambert-Eaton Myasthenic Syndrome Dr. SitoyNeil Victor Ongco PajugotNessuna valutazione finora
- Definition of TermssDocumento8 pagineDefinition of TermssMariel AbatayoNessuna valutazione finora
- Myasthenia Gravis Lecture 12Documento59 pagineMyasthenia Gravis Lecture 12Pop D. MadalinaNessuna valutazione finora
- Myasthenia Gravis: 50 year old male with difficulty walking and standingDocumento44 pagineMyasthenia Gravis: 50 year old male with difficulty walking and standingAli KhaqaanNessuna valutazione finora
- Source 3Documento3 pagineSource 3PJHGNessuna valutazione finora
- Group 1 Seizure DisordersDocumento13 pagineGroup 1 Seizure DisordersDiana MurguiaNessuna valutazione finora
- Disorder of Neuromuscular Junction: Myasthenia Gravis and Lambert-Eaton Myasthenic SyndromeDocumento36 pagineDisorder of Neuromuscular Junction: Myasthenia Gravis and Lambert-Eaton Myasthenic SyndromePraneethaNessuna valutazione finora
- Myasthenia Gravis: by Neha Mhapralkar MSCBT 12015Documento20 pagineMyasthenia Gravis: by Neha Mhapralkar MSCBT 12015Neha MhapralkarNessuna valutazione finora
- Neuromuscular Junction DisordersDocumento32 pagineNeuromuscular Junction Disordersepic sound everNessuna valutazione finora
- Status Epilepticus GuideDocumento10 pagineStatus Epilepticus GuideGladys MainaNessuna valutazione finora
- Myasthenia GravisDocumento18 pagineMyasthenia GravisvandanaNessuna valutazione finora
- Wa0033.Documento14 pagineWa0033.Irb azNessuna valutazione finora
- Myasthenia Gravis: Assoc. Prof. Dr. Rodica BălașaDocumento31 pagineMyasthenia Gravis: Assoc. Prof. Dr. Rodica BălașaIstván MáthéNessuna valutazione finora
- Laporan Kasus: Myasthenia GravisDocumento41 pagineLaporan Kasus: Myasthenia GravisTias DiahNessuna valutazione finora
- Autoimmune Disorders of Central Nervous System: Lutsenko I.LDocumento46 pagineAutoimmune Disorders of Central Nervous System: Lutsenko I.LDrhikmatullah SheraniNessuna valutazione finora
- Myasthenia Gravis: Dr. Ken Wirastuti, Mkes, SP.S Bagian Ilmu Penyakit Saraf Fk. UnissulaDocumento30 pagineMyasthenia Gravis: Dr. Ken Wirastuti, Mkes, SP.S Bagian Ilmu Penyakit Saraf Fk. UnissulafemmytaniaNessuna valutazione finora
- Neuromuscular Junction Disorders ExplainedDocumento24 pagineNeuromuscular Junction Disorders ExplainedMaluNessuna valutazione finora
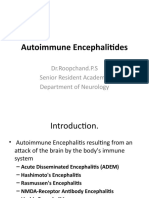
- Autoimmuneencephalitides 130623114238 Phpapp01Documento21 pagineAutoimmuneencephalitides 130623114238 Phpapp01Tamer El GoharyNessuna valutazione finora
- Autoimmune Encephalitis 3Documento27 pagineAutoimmune Encephalitis 3Majid UllahNessuna valutazione finora
- Myasthenia Gravis, Alzheimers Disease, Multiple Sclerosis, Guillain-Barre Syndrome and Bell PalsyDocumento9 pagineMyasthenia Gravis, Alzheimers Disease, Multiple Sclerosis, Guillain-Barre Syndrome and Bell PalsyNielArmstrongNessuna valutazione finora
- Plasma Cell DyscrasiasDocumento68 paginePlasma Cell Dyscrasiassarath chandranNessuna valutazione finora
- Board Study NotesDocumento44 pagineBoard Study Notesrcrdvg93Nessuna valutazione finora
- Case 1Documento12 pagineCase 1Denisa-Alexandra MănăstireanuNessuna valutazione finora
- Anaesthesia and Myasthenia GravisDocumento12 pagineAnaesthesia and Myasthenia Gravis37435rlcNessuna valutazione finora
- Referat MG Desya BismillahDocumento20 pagineReferat MG Desya BismillahDesya BillaNessuna valutazione finora
- Toxoplasmosis in HIV PatientsDocumento49 pagineToxoplasmosis in HIV PatientsLily SolNessuna valutazione finora
- Myasthenia Gravis: Susan Hotz, M.D. Medical City Dallas Hospital Dallas, TexasDocumento26 pagineMyasthenia Gravis: Susan Hotz, M.D. Medical City Dallas Hospital Dallas, TexasErdina putriNessuna valutazione finora
- Myasthenia Gravis: Moderator: DR Anitha PG: DR VijethaDocumento45 pagineMyasthenia Gravis: Moderator: DR Anitha PG: DR VijethaJerusha VijethaNessuna valutazione finora
- Autoimmune EncephalitisDocumento11 pagineAutoimmune Encephalitisbamboo snooksNessuna valutazione finora
- Saraf 8Documento141 pagineSaraf 8Vivian SaputraNessuna valutazione finora
- Disorders of The Neuromuscular Junction: Myasthenia GravisDocumento7 pagineDisorders of The Neuromuscular Junction: Myasthenia GravisZain AlAbideen AlTaeeNessuna valutazione finora
- Motor Endplate Disorders Myasthenia Gravis Overview and DefinitionDocumento4 pagineMotor Endplate Disorders Myasthenia Gravis Overview and DefinitionPJHGNessuna valutazione finora
- Myasthenia GravisDocumento31 pagineMyasthenia Gravisjsampsonemtp100% (2)
- Neurological EmergenciesDocumento47 pagineNeurological EmergenciesStellate Repentance100% (1)
- Autoimmune Disorder Causing Muscle WeaknessDocumento2 pagineAutoimmune Disorder Causing Muscle Weaknessnicdeep100% (1)
- 2 Myasthenia Gravis and MS 2Documento50 pagine2 Myasthenia Gravis and MS 2Rawbeena RamtelNessuna valutazione finora
- Neuromuscular Disorders in ICUDocumento82 pagineNeuromuscular Disorders in ICUCutie PieNessuna valutazione finora
- Case Presentation and Review of LiteratureDocumento65 pagineCase Presentation and Review of LiteratureShrey BhatlaNessuna valutazione finora
- Myasthenia GravisDocumento25 pagineMyasthenia GravisPriyadharshini BalanNessuna valutazione finora
- Myasthenia GravisDocumento32 pagineMyasthenia GravisSandhya HarbolaNessuna valutazione finora
- PBL 10Documento4 paginePBL 10lliioNessuna valutazione finora
- Weekly Presentation and Discussion On Systemic Lupus Erythematosus (Sle)Documento59 pagineWeekly Presentation and Discussion On Systemic Lupus Erythematosus (Sle)Dr AnilNessuna valutazione finora
- Neuromuscular DisordersDocumento3 pagineNeuromuscular DisordersMaharaniDewiNessuna valutazione finora
- EPILEPSY AND ANTI-EPILEPTIC DRUGS For PresentationDocumento91 pagineEPILEPSY AND ANTI-EPILEPTIC DRUGS For PresentationKenneth NuñezNessuna valutazione finora
- Epilepsy: DR Hammad Ur Rehman Bhatti Assistant ProfessorDocumento19 pagineEpilepsy: DR Hammad Ur Rehman Bhatti Assistant ProfessorarshmeentariqNessuna valutazione finora
- Paraneoplastic Neurologic Syndromes Are Defined and Characterized by An Inappropriate Immune Response Targeting Native Nervous System Antigens That Are Ectopically Expressed by A Systemic TumorDocumento11 pagineParaneoplastic Neurologic Syndromes Are Defined and Characterized by An Inappropriate Immune Response Targeting Native Nervous System Antigens That Are Ectopically Expressed by A Systemic TumorAnonymous ZUaUz1wwNessuna valutazione finora
- Transverse MyelitisDocumento16 pagineTransverse MyelitisahmicphdNessuna valutazione finora
- Epilepsy: Neurovascular DisordersDocumento30 pagineEpilepsy: Neurovascular DisordersNdoo NdooNessuna valutazione finora
- Paraneoplastic Disorders of the Central Nervous SystemDocumento71 pagineParaneoplastic Disorders of the Central Nervous Systempreeti sharmaNessuna valutazione finora
- Myasthenia Gravis: MG-epidemiologyDocumento3 pagineMyasthenia Gravis: MG-epidemiologyRemigius RiyanNessuna valutazione finora
- Resident morning report on 60yo male with Bickerstaff encephalitisDocumento21 pagineResident morning report on 60yo male with Bickerstaff encephalitisAng LiNessuna valutazione finora
- Neuromuscular Junction Disorders: Applied AnatomyDocumento6 pagineNeuromuscular Junction Disorders: Applied Anatomyspicychips7Nessuna valutazione finora
- Neurologija SkripticaDocumento26 pagineNeurologija SkripticaLazar VučetićNessuna valutazione finora
- Neuromuscular DisordersDocumento8 pagineNeuromuscular DisordersShauki AliNessuna valutazione finora
- Malignant Hyperthermia: Presentation By: DR Ramanesh Mageswaran Hospital Kuala LumpurDocumento41 pagineMalignant Hyperthermia: Presentation By: DR Ramanesh Mageswaran Hospital Kuala LumpuranaeshklNessuna valutazione finora
- NML 4an3b DiscussionDocumento17 pagineNML 4an3b DiscussionSheana TmplNessuna valutazione finora
- Drug Name Action Indication Contraindication Side Effects Nursing ResponsibilitiesDocumento1 paginaDrug Name Action Indication Contraindication Side Effects Nursing ResponsibilitiesSheana TmplNessuna valutazione finora
- Drug Name Action Indication Contraindication Side Effects Nursing ResponsibilitiesDocumento1 paginaDrug Name Action Indication Contraindication Side Effects Nursing ResponsibilitiesSheana TmplNessuna valutazione finora
- Pareto ChartDocumento1 paginaPareto ChartSheana TmplNessuna valutazione finora
- Nursing TheoriesDocumento2 pagineNursing TheoriesSheana TmplNessuna valutazione finora
- Elective II ReviewerDocumento4 pagineElective II ReviewerSheana TmplNessuna valutazione finora
- Performance Improvement ToolsDocumento5 paginePerformance Improvement ToolsSheana TmplNessuna valutazione finora
- Pareto ChartDocumento1 paginaPareto ChartSheana TmplNessuna valutazione finora
- DSA worksheet guides quality improvement cyclesDocumento7 pagineDSA worksheet guides quality improvement cyclesSheana TmplNessuna valutazione finora
- GYNECOLOGICALNURSINGDocumento4 pagineGYNECOLOGICALNURSINGSheana TmplNessuna valutazione finora
- ManualDocumento9 pagineManualSheana TmplNessuna valutazione finora
- Common Surgical Procedure1Documento4 pagineCommon Surgical Procedure1Sheana TmplNessuna valutazione finora
- Elective IIDocumento13 pagineElective IISheana TmplNessuna valutazione finora
- DSA worksheet guides quality improvement cyclesDocumento7 pagineDSA worksheet guides quality improvement cyclesSheana TmplNessuna valutazione finora
- NCPDocumento3 pagineNCPSheana TmplNessuna valutazione finora
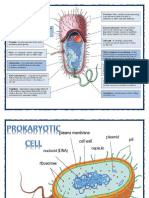
- Prokaryotic CellDocumento2 pagineProkaryotic CellSheana TmplNessuna valutazione finora
- ObjectivesDocumento2 pagineObjectivesSheana TmplNessuna valutazione finora
- Review Eeee ErDocumento8 pagineReview Eeee ErSheana TmplNessuna valutazione finora
- Group QuestionsDocumento7 pagineGroup QuestionsSheana TmplNessuna valutazione finora
- Nursing HistoryDocumento2 pagineNursing HistorySheana TmplNessuna valutazione finora
- Walang LamanDocumento1 paginaWalang LamanSheana TmplNessuna valutazione finora
- First ENCD Youth RallyDocumento1 paginaFirst ENCD Youth RallySheana TmplNessuna valutazione finora
- 220/132 KV Sub-Station Bhilai-3: Training Report ONDocumento24 pagine220/132 KV Sub-Station Bhilai-3: Training Report ONKalyani ShuklaNessuna valutazione finora
- Secondary AssessmentsDocumento12 pagineSecondary Assessmentsapi-338389967Nessuna valutazione finora
- Kootenay Lake Pennywise October 17, 2017Documento40 pagineKootenay Lake Pennywise October 17, 2017Pennywise PublishingNessuna valutazione finora
- EXPERIMENT 5 - Chroamtorgraphy GRP9 RevDocumento2 pagineEXPERIMENT 5 - Chroamtorgraphy GRP9 RevMic100% (2)
- Biosafety FH Guidance Guide Good Manufacturing Practice enDocumento40 pagineBiosafety FH Guidance Guide Good Manufacturing Practice enMaritsa PerHerNessuna valutazione finora
- Refresher 2 (Pipe)Documento12 pagineRefresher 2 (Pipe)Kira YagamiNessuna valutazione finora
- Environmental Product Declaration: PU EuropeDocumento6 pagineEnvironmental Product Declaration: PU EuropeIngeniero Mac DonnellNessuna valutazione finora
- 2005-05-12Documento18 pagine2005-05-12The University Daily KansanNessuna valutazione finora
- Flexible and Alternative Seating: in ClassroomsDocumento5 pagineFlexible and Alternative Seating: in ClassroomsweningNessuna valutazione finora
- Sunflower Herbicide ChartDocumento2 pagineSunflower Herbicide ChartpapucicaNessuna valutazione finora
- 1324 1624 1824 Owners Manual 6 4 08Documento64 pagine1324 1624 1824 Owners Manual 6 4 08Miguel LopNessuna valutazione finora
- CSK - W - My - Mother - at - Sixty - Six 2Documento2 pagineCSK - W - My - Mother - at - Sixty - Six 2Aaron JoshiNessuna valutazione finora
- Ficha Tecnica Emeral 8C PDFDocumento11 pagineFicha Tecnica Emeral 8C PDFLeticia KoerichNessuna valutazione finora
- IC 33 Question PaperDocumento12 pagineIC 33 Question PaperSushil MehraNessuna valutazione finora
- Steroids ActivityDocumento1 paginaSteroids Activityfaqed ilzakiraNessuna valutazione finora
- Eu Donor Atlas PDFDocumento2 pagineEu Donor Atlas PDFBrentNessuna valutazione finora
- Final Profile Draft - Zach HelfantDocumento5 pagineFinal Profile Draft - Zach Helfantapi-547420544Nessuna valutazione finora
- Liquid - Liquid ExtractionDocumento19 pagineLiquid - Liquid ExtractionApurba Sarker ApuNessuna valutazione finora
- Smart Goals ExerciseDocumento2 pagineSmart Goals Exerciseapi-594661640Nessuna valutazione finora
- Afforestation in Arid and Semi Arid RegionsDocumento68 pagineAfforestation in Arid and Semi Arid RegionsMilian Marian SanduNessuna valutazione finora
- Regional Ecology Test ScoringDocumento14 pagineRegional Ecology Test Scoringaisyah Wardah201Nessuna valutazione finora
- Heat Transfer Augmentation in Decaying Turbulent Swirl FlowDocumento1 paginaHeat Transfer Augmentation in Decaying Turbulent Swirl FlowOnkar ChavanNessuna valutazione finora