Potrebbero piacerti anche
- MM Fun Run June 11 - Race Release FormDocumento1 paginaMM Fun Run June 11 - Race Release Formapi-237868140Nessuna valutazione finora
- HC 2013 Release Form - 0Documento1 paginaHC 2013 Release Form - 0Ted MaoNessuna valutazione finora
- Intersession PermissionDocumento2 pagineIntersession PermissionMatt PatrickNessuna valutazione finora
- University of Agriculture, Faisalabad: Application Form For Admission ToDocumento2 pagineUniversity of Agriculture, Faisalabad: Application Form For Admission ToMoodserNessuna valutazione finora
- Release, Indemnity and Legal Concealed Carry, LLC Course AgreementDocumento2 pagineRelease, Indemnity and Legal Concealed Carry, LLC Course AgreementGio RatnaclaNessuna valutazione finora
- Q&A: Sexual Harassment Cases in the WorkplaceDocumento16 pagineQ&A: Sexual Harassment Cases in the WorkplaceCarla Blanca MaisoNessuna valutazione finora
- Q & A: Sexual Harassment CasesDocumento9 pagineQ & A: Sexual Harassment CasesZahjid CallangNessuna valutazione finora
- Francis Christopher Hall, CPP, Pci 1843 Sweetwood Drive DALY CITY, CALIFORNIA 94015-2014 TELEPHONE: (650) 278-0790Documento5 pagineFrancis Christopher Hall, CPP, Pci 1843 Sweetwood Drive DALY CITY, CALIFORNIA 94015-2014 TELEPHONE: (650) 278-0790francischall10350% (1)
- RA 7877 PresentationDocumento27 pagineRA 7877 PresentationprincessNessuna valutazione finora
- SR - Rape and Sexual OffensesDocumento38 pagineSR - Rape and Sexual OffensesAlbert Remollo JrNessuna valutazione finora
- Humber Midnight Madness 2011Documento2 pagineHumber Midnight Madness 2011Kenny NgNessuna valutazione finora
- UntitledDocumento3 pagineUntitledapi-77142148Nessuna valutazione finora
- Discrimination Grievance Procedures Purpose: Eoaa@umontana - Edu WWW - Umt.edu/eoDocumento12 pagineDiscrimination Grievance Procedures Purpose: Eoaa@umontana - Edu WWW - Umt.edu/eoFIRENessuna valutazione finora
- 2015 Individual Waiver FormDocumento2 pagine2015 Individual Waiver FormAlinaUtrataNessuna valutazione finora
- Register for 2014 Northeast College TourDocumento4 pagineRegister for 2014 Northeast College TourOzzy WeliNessuna valutazione finora
- Denver Public Schools Policy GBA-R1: Procedures For The Investigation of Employee Complaints of Discrimination or HarassmentDocumento5 pagineDenver Public Schools Policy GBA-R1: Procedures For The Investigation of Employee Complaints of Discrimination or HarassmentMichael_Lee_RobertsNessuna valutazione finora
- 503 4arDocumento8 pagine503 4arapi-287922045Nessuna valutazione finora
- IBPS .Model Code of Conduct For SARTHI Sponsored CandidateDocumento3 pagineIBPS .Model Code of Conduct For SARTHI Sponsored CandidateOM JADHAVNessuna valutazione finora
- Application FormDocumento1 paginaApplication FormAkshat AtrayNessuna valutazione finora
- Ra 6981Documento17 pagineRa 6981Michelle Quiquino FolienteNessuna valutazione finora
- Jersey's Fastest Entry FormDocumento5 pagineJersey's Fastest Entry Form08hillrNessuna valutazione finora
- 2018 Performing Arts Project Waiver and Release FormDocumento1 pagina2018 Performing Arts Project Waiver and Release FormVaibu MohanNessuna valutazione finora
- 2023 Florida Relays High School Meet InfoDocumento6 pagine2023 Florida Relays High School Meet InfoAshley TysiacNessuna valutazione finora
- Walker Registration FormDocumento1 paginaWalker Registration FormKendra SikesNessuna valutazione finora
- Safe Spaces ActDocumento12 pagineSafe Spaces ActRichie SalubreNessuna valutazione finora
- CODI Rules on Sexual Harassment CasesDocumento80 pagineCODI Rules on Sexual Harassment CasesJRMSU Finance OfficeNessuna valutazione finora
- Investigations of Staff MembersDocumento5 pagineInvestigations of Staff MembersParents' Coalition of Montgomery County, MarylandNessuna valutazione finora
- Lldlplayerregistrationformfinal DraftDocumento1 paginaLldlplayerregistrationformfinal Draftapi-200598193Nessuna valutazione finora
- Sexual HarrassmentDocumento33 pagineSexual Harrassmentrida merleNessuna valutazione finora
- 50+ Games Entry FormDocumento1 pagina50+ Games Entry FormVanessa VaileNessuna valutazione finora
- 2.5 Day Tactical Pistol HandbookDocumento31 pagine2.5 Day Tactical Pistol Handbookshotgun1897100% (2)
- TR98 C&S Day Enrolment FormDocumento2 pagineTR98 C&S Day Enrolment FormTiffany ChapmanNessuna valutazione finora
- CODI On Sexual Harassment CasesDocumento39 pagineCODI On Sexual Harassment CasesDeniel Salvador B. MorilloNessuna valutazione finora
- 5K WaiverDocumento1 pagina5K WaiverPAOLO DAVIDNessuna valutazione finora
- Dance Permission SlipDocumento1 paginaDance Permission SlipRebecca YamamotoNessuna valutazione finora
- Joint Undertaking New StudentsDocumento2 pagineJoint Undertaking New StudentsAbhiram KunchapuNessuna valutazione finora
- Athlete Waiver Form for SEAG OCR EventsDocumento2 pagineAthlete Waiver Form for SEAG OCR EventsChaz Garcia-AnganNessuna valutazione finora
- TourDeFranzia RegSheet 2011Documento2 pagineTourDeFranzia RegSheet 2011andria_amenNessuna valutazione finora
- Operating Procedure 3.8 Response To Sexual Assault CasesDocumento4 pagineOperating Procedure 3.8 Response To Sexual Assault CasesAdam BoothNessuna valutazione finora
- Letter of Undertaking by Students: TH NDDocumento1 paginaLetter of Undertaking by Students: TH NDArun C DixitNessuna valutazione finora
- Hall Ticket Exam DetailsDocumento1 paginaHall Ticket Exam Detailskarthiraja_1981Nessuna valutazione finora
- Application FormDocumento1 paginaApplication FormNitin GuptaNessuna valutazione finora
- Charleston Police Dept. Citizens Police Academy Application: Print FormDocumento1 paginaCharleston Police Dept. Citizens Police Academy Application: Print FormJeff MorrisNessuna valutazione finora
- Anti Ragging CommitieeDocumento3 pagineAnti Ragging CommitieeAniket SankpalNessuna valutazione finora
- This Form Must Be Completed To Be Considered For Employment: Conviction/Criminal History InformationDocumento1 paginaThis Form Must Be Completed To Be Considered For Employment: Conviction/Criminal History InformationRICK STANTONNessuna valutazione finora
- Abuse and Neglect PolicyDocumento4 pagineAbuse and Neglect PolicyRhodora BenipayoNessuna valutazione finora
- Amazing Race: Eastern Shore Edition WaiverDocumento5 pagineAmazing Race: Eastern Shore Edition WaiverDylan KemperNessuna valutazione finora
- Crimson Talon Track Club Summer 2016 BrochureDocumento4 pagineCrimson Talon Track Club Summer 2016 Brochureapi-252046491Nessuna valutazione finora
- Sexual HarassmentDocumento74 pagineSexual Harassmentannejerebajarias100% (1)
- Release FormDocumento1 paginaRelease FormMV Sai KiranNessuna valutazione finora
- Q and A On SEXUAL HArassmentDocumento42 pagineQ and A On SEXUAL HArassmentEJ FabrigaNessuna valutazione finora
- Field Trip ContractDocumento3 pagineField Trip ContractAfeefah AllyNessuna valutazione finora
- Allure WavierDocumento1 paginaAllure Wavierapi-271089940Nessuna valutazione finora
- California Survival School Release and Waiver Agreement 2018 PDFDocumento2 pagineCalifornia Survival School Release and Waiver Agreement 2018 PDFAnonymous zhNqC0KmmNessuna valutazione finora
- Local Educational Tour Waiver FormDocumento1 paginaLocal Educational Tour Waiver FormJohann GreiNessuna valutazione finora
- SOSD Volunteer Registration & Indemnity FormDocumento2 pagineSOSD Volunteer Registration & Indemnity FormChasity WilliamsNessuna valutazione finora
- United States Special Army Cadets Application and Enrollment AgreementDocumento3 pagineUnited States Special Army Cadets Application and Enrollment AgreementFrancisco MillanNessuna valutazione finora
- Doubles Pickleball Round Robin 031216 2Documento2 pagineDoubles Pickleball Round Robin 031216 2saukvalleynewsNessuna valutazione finora
- Revised Administrative Disciplinary Rules On Sexual Harassment CasesDocumento65 pagineRevised Administrative Disciplinary Rules On Sexual Harassment CasesJem Cromwell S. Gorospe100% (1)
- Blackbeard's Cannons Reveal Pirate Ship MysteryDocumento2 pagineBlackbeard's Cannons Reveal Pirate Ship MysteryJean Marie CruzNessuna valutazione finora
- Ged117 - Final ExamDocumento3 pagineGed117 - Final ExamLed ArmorNessuna valutazione finora
- Powder Bushing: ChartDocumento2 paginePowder Bushing: Chartmikeabramson316Nessuna valutazione finora
- Melanie Phillips and IranDocumento5 pagineMelanie Phillips and IranBinamAryaniNessuna valutazione finora
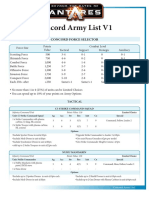
- Beyond The Gates of Antares Concord Army ListsDocumento7 pagineBeyond The Gates of Antares Concord Army ListsDavid HuntNessuna valutazione finora
- Datasheet Eldar Phantom TitanDocumento1 paginaDatasheet Eldar Phantom Titangordy2000Nessuna valutazione finora
- Sample Rocketry Questions ExplainedDocumento6 pagineSample Rocketry Questions ExplainedAdetoro Mal PascalNessuna valutazione finora
- FM 71-2 Tank/Mech Battalion 1972Documento370 pagineFM 71-2 Tank/Mech Battalion 1972Charles Junior100% (2)
- Gatka - Wikipedia PDFDocumento16 pagineGatka - Wikipedia PDFGurdeepsingh SinghNessuna valutazione finora
- RAN Working Paper No.2Documento19 pagineRAN Working Paper No.2Rex TyrannosaurNessuna valutazione finora
- Modern Alchemist Nicholas de ColletteDocumento8 pagineModern Alchemist Nicholas de ColletteLaron Clark50% (2)
- GN1 Overlock Machine Manual in English PDFDocumento23 pagineGN1 Overlock Machine Manual in English PDFomaramedNessuna valutazione finora
- Eh Errata Faq 2017-08-11Documento11 pagineEh Errata Faq 2017-08-11Ron PzVieNessuna valutazione finora
- Ammunition GeneralDocumento243 pagineAmmunition GeneralPlainNormalGuy2100% (4)
- Artillery TrendsDocumento89 pagineArtillery Trendstheduck666Nessuna valutazione finora
- Wild ArmsDocumento157 pagineWild ArmsRayon DahaNessuna valutazione finora
- My Brothers Road by Melkonian, Markar Seta Melkonian Z Lib OrgDocumento343 pagineMy Brothers Road by Melkonian, Markar Seta Melkonian Z Lib Orghappy doge channelNessuna valutazione finora
- Inxrecon - Print at HomeDocumento12 pagineInxrecon - Print at HomeJMNessuna valutazione finora
- Warhammer - The Laughter of Dark Gods by David Pringle (Ed) (Undead) (v1.0)Documento162 pagineWarhammer - The Laughter of Dark Gods by David Pringle (Ed) (Undead) (v1.0)jmacdonaldross100% (3)
- Packing The TornisterDocumento19 paginePacking The TornisterManfred FischerNessuna valutazione finora
- Circleofnoms TOR 2e Homebrew CollectionDocumento390 pagineCircleofnoms TOR 2e Homebrew CollectionYves Lapierre100% (1)
- Thanos BiographyDocumento2 pagineThanos Biographyapi-348836713Nessuna valutazione finora
- Witcher Easy ModeDocumento32 pagineWitcher Easy ModeFelipe Oliveira100% (3)
- Bad Boys The British Rifle, Anti-Tank, .55 In, BoysDocumento15 pagineBad Boys The British Rifle, Anti-Tank, .55 In, BoysBob CashnerNessuna valutazione finora
- French XIII Corps (Hamburg), Mid-August 1813Documento3 pagineFrench XIII Corps (Hamburg), Mid-August 1813airfix1999Nessuna valutazione finora
- 86-EIGHTY-SIX, Vol. 2Documento187 pagine86-EIGHTY-SIX, Vol. 2Neetu KatiyarNessuna valutazione finora
- Open Legend RPG Core Rule BookDocumento293 pagineOpen Legend RPG Core Rule BookPeter Jackson100% (1)
- TOW Weapon System - FM 23-34Documento313 pagineTOW Weapon System - FM 23-34Andriamahefamanana Onja TantelyNessuna valutazione finora
- Learn Carbine BasicsDocumento15 pagineLearn Carbine BasicsAnonymous mcJZ1wVX89Nessuna valutazione finora