Potrebbero piacerti anche
- Exercise and Myasthenia Gravis (MG)Documento3 pagineExercise and Myasthenia Gravis (MG)sridhar_physioNessuna valutazione finora
- Movement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementDa EverandMovement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementNessuna valutazione finora
- .Scapular StabilityDocumento5 pagine.Scapular StabilityEileen Torres Cerda100% (1)
- Post Partum Care: Care Within The First 24 HoursDocumento4 paginePost Partum Care: Care Within The First 24 HoursCarrie ANessuna valutazione finora
- Toe Touch ProgressionDocumento1 paginaToe Touch Progressionses1984205Nessuna valutazione finora
- Anterior Shoulder DislocationDocumento2 pagineAnterior Shoulder DislocationcilengsaiNessuna valutazione finora
- Deepak Panwar Bachelor of Physiotherapy, School of Physiotherapy, Delhi Pharmaceutical Sciences & Research UniversityDocumento1 paginaDeepak Panwar Bachelor of Physiotherapy, School of Physiotherapy, Delhi Pharmaceutical Sciences & Research UniversityAsad AnZariNessuna valutazione finora
- What Is Biceps Tendonitis?Documento5 pagineWhat Is Biceps Tendonitis?Nishant RajaNessuna valutazione finora
- Warm Up PDFDocumento6 pagineWarm Up PDFBraga DanNessuna valutazione finora
- Tennis Elbow PDFDocumento2 pagineTennis Elbow PDFSabau PetreNessuna valutazione finora
- PIN2763 Thoracic Spine ExercisesDocumento3 paginePIN2763 Thoracic Spine ExercisesShamsuddin Hasnani100% (1)
- Cervical Spondylosis and Neck PainDocumento5 pagineCervical Spondylosis and Neck PainIsaac AlemanNessuna valutazione finora
- Spinal Cord BasicsDocumento2 pagineSpinal Cord BasicscpradheepNessuna valutazione finora
- The Guideline For Standing SCI Mascip FinalDocumento30 pagineThe Guideline For Standing SCI Mascip FinalJavierSanMartínHerreraNessuna valutazione finora
- Post Natal ExercisesDocumento7 paginePost Natal ExercisesEvie Dolpin BlueNessuna valutazione finora
- Human Anatomy & PhysiologyDocumento72 pagineHuman Anatomy & PhysiologyJoie UrsalNessuna valutazione finora
- Patient Leaflet DeQuervains PDFDocumento5 paginePatient Leaflet DeQuervains PDFDimas SatyaNessuna valutazione finora
- Vojta Self Training Experiences of Six Neurologically Impaired People A Qualitative Study 2000 PhysiotherapyDocumento8 pagineVojta Self Training Experiences of Six Neurologically Impaired People A Qualitative Study 2000 PhysiotherapyJose J.100% (1)
- Rib Cage CoursesDocumento11 pagineRib Cage CoursesPBNessuna valutazione finora
- Post Natal ExercisesDocumento12 paginePost Natal ExercisesDeepika SensuaNessuna valutazione finora
- Physio Following Your Gynaecological OperationDocumento10 paginePhysio Following Your Gynaecological OperationSoum Subhra SahaNessuna valutazione finora
- HyperLordosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHyperLordosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- MICB4454 Metacarpal Fracture PDFDocumento2 pagineMICB4454 Metacarpal Fracture PDFZakiyuddin FathoniNessuna valutazione finora
- Pregnancy-Related Pelvic Girdle Pain: Second Stage of LabourDocumento4 paginePregnancy-Related Pelvic Girdle Pain: Second Stage of LabourSravan Ganji100% (1)
- Rotator Cuff Syndrome GuidelinesDocumento84 pagineRotator Cuff Syndrome GuidelinesAnjatNessuna valutazione finora
- Post Stroke Functional Exercises For RehabilitationDocumento37 paginePost Stroke Functional Exercises For Rehabilitationjoel_simon_23100% (1)
- Physiotherapy For Osteoarthritis of The Knee PDFDocumento391 paginePhysiotherapy For Osteoarthritis of The Knee PDFPipi KNessuna valutazione finora
- Jurnal Frozen ShoulderDocumento21 pagineJurnal Frozen ShoulderMega Mulya Dwi FitriyaniNessuna valutazione finora
- PreConception Care 4 Student VersionDocumento38 paginePreConception Care 4 Student VersionKajal SinghNessuna valutazione finora
- HEP2GO Carpal Tunnel Program PDFDocumento2 pagineHEP2GO Carpal Tunnel Program PDFBetty OberackerNessuna valutazione finora
- Disk HerniationDocumento27 pagineDisk HerniationDamiati78Nessuna valutazione finora
- Physio After SurgeryDocumento2 paginePhysio After SurgeryGursangeet KaurNessuna valutazione finora
- Enhancing the Benefits of Nauli with a Key Exercise for Abdominal Muscle StrengthDa EverandEnhancing the Benefits of Nauli with a Key Exercise for Abdominal Muscle StrengthValutazione: 5 su 5 stelle5/5 (1)
- Physiotherapy and Frozen ShoulderDocumento7 paginePhysiotherapy and Frozen Shoulderdeepa1982Nessuna valutazione finora
- 429 FT0 Physiotherapy in Obstetrics Gynaecology Mohd. JavedDocumento86 pagine429 FT0 Physiotherapy in Obstetrics Gynaecology Mohd. JavedRekha Satheesan100% (1)
- Yoga for Beginners: Prenatal Yoga: With the Convenience of Doing Prenatal Yoga at Home!!Da EverandYoga for Beginners: Prenatal Yoga: With the Convenience of Doing Prenatal Yoga at Home!!Nessuna valutazione finora
- Balance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementDa EverandBalance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementNessuna valutazione finora
- Acute and Chronic PainDocumento20 pagineAcute and Chronic PainsukunathNessuna valutazione finora
- Low Back PainDocumento81 pagineLow Back PainFacu YaneNessuna valutazione finora
- Coccyx Pain Following Childbirth - Oct20Documento6 pagineCoccyx Pain Following Childbirth - Oct20PofNessuna valutazione finora
- Assessment of Back Pain-BMJDocumento30 pagineAssessment of Back Pain-BMJMarco Paulo Reyes NaoeNessuna valutazione finora
- Post Natal ExercisesDocumento4 paginePost Natal ExercisesnurasyikahNessuna valutazione finora
- Bells Palsy Management in AdultsDocumento8 pagineBells Palsy Management in Adultsnur fajri rahmiNessuna valutazione finora
- Physiotherapy Based On The Bobath ConceptpdfDocumento6 paginePhysiotherapy Based On The Bobath ConceptpdfmatsNessuna valutazione finora
- Special Tests of The Hip & Pelvis: Kendall TestDocumento5 pagineSpecial Tests of The Hip & Pelvis: Kendall Testsungmin kimNessuna valutazione finora
- Motor Control ListDocumento18 pagineMotor Control Listsridhar_physioNessuna valutazione finora
- Fracture Colles Wrist Exercise-AfterDocumento4 pagineFracture Colles Wrist Exercise-Afterfaprilisa100% (1)
- Exercise your way to health: Arthritis: Exercise plans to improve your lifeDa EverandExercise your way to health: Arthritis: Exercise plans to improve your lifeNessuna valutazione finora
- Failure of Weaning:: According To The European Respiratory Society (ERS) Task ForceDocumento12 pagineFailure of Weaning:: According To The European Respiratory Society (ERS) Task ForceAmr El Taher0% (1)
- The Stranger Comes at Sundown: Living & Dying with Parkinson's DiseaseDa EverandThe Stranger Comes at Sundown: Living & Dying with Parkinson's DiseaseValutazione: 3 su 5 stelle3/5 (1)
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Good Posture and Postural DeformitiesDocumento13 pagineGood Posture and Postural DeformitiesAnne NashNessuna valutazione finora
- Contemporary Issues in Occupational Therapy: Reasoning and ReflectionDa EverandContemporary Issues in Occupational Therapy: Reasoning and ReflectionNessuna valutazione finora
- Posterior Cruciate Ligament (PCLR) Rehabilitation ProtocolDocumento19 paginePosterior Cruciate Ligament (PCLR) Rehabilitation ProtocolosamadrNessuna valutazione finora
- PT - Spasticity in Cerebral PalsyDocumento103 paginePT - Spasticity in Cerebral PalsysandeepNessuna valutazione finora
- Shoulder InjuryDocumento79 pagineShoulder InjurySudipta BhowmickNessuna valutazione finora
- MAT ProgressionDocumento1 paginaMAT ProgressionshodhgangaNessuna valutazione finora
- Gross Motor Function MeasureDocumento95 pagineGross Motor Function MeasureshodhgangaNessuna valutazione finora
- SyringomyeliaDocumento9 pagineSyringomyeliashodhgangaNessuna valutazione finora
- Brazilian Journal of Physical TherapyDocumento11 pagineBrazilian Journal of Physical TherapyshodhgangaNessuna valutazione finora
- Research in Developmental DisabilitiesDocumento6 pagineResearch in Developmental DisabilitiesshodhgangaNessuna valutazione finora
- An Approach To The Design of Wheelchairs For Young UsersDocumento5 pagineAn Approach To The Design of Wheelchairs For Young UsersshodhgangaNessuna valutazione finora
- Use of The Hammersmith Infant Neurological Examination in Infants With Cerebral Palsy: A Critical Review of The LiteratureDocumento6 pagineUse of The Hammersmith Infant Neurological Examination in Infants With Cerebral Palsy: A Critical Review of The LiteratureshodhgangaNessuna valutazione finora
- The Twisting Force of Aged Consumers When Opening A JarDocumento5 pagineThe Twisting Force of Aged Consumers When Opening A JarshodhgangaNessuna valutazione finora
- Role of Corticotropin-Releasing Factor in Cerebellar Motor Control and AtaxiaDocumento15 pagineRole of Corticotropin-Releasing Factor in Cerebellar Motor Control and AtaxiashodhgangaNessuna valutazione finora
- Aphasia, Memory and Cerebral DisordersDocumento15 pagineAphasia, Memory and Cerebral DisordersshodhgangaNessuna valutazione finora
- Muscle Weakness and Functional Disability in Patients With Myasthenia GravisDocumento6 pagineMuscle Weakness and Functional Disability in Patients With Myasthenia GravisshodhgangaNessuna valutazione finora
- Neurological Assessment ChartDocumento5 pagineNeurological Assessment ChartshodhgangaNessuna valutazione finora
- The Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseDocumento9 pagineThe Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseshodhgangaNessuna valutazione finora
- Developmental Review: T. Gliga, E.J.H. Jones, R. Bedford, T. Charman, M.H. JohnsonDocumento19 pagineDevelopmental Review: T. Gliga, E.J.H. Jones, R. Bedford, T. Charman, M.H. JohnsonshodhgangaNessuna valutazione finora
- The Influence of Initial Posture On The Sit-To-Stand MovementDocumento6 pagineThe Influence of Initial Posture On The Sit-To-Stand MovementshodhgangaNessuna valutazione finora
- Facial Nerve Examination OnlyDocumento17 pagineFacial Nerve Examination OnlyshodhgangaNessuna valutazione finora
- Muscle Force and Range of Motion Predictors of Balance in CPDocumento21 pagineMuscle Force and Range of Motion Predictors of Balance in CPshodhgangaNessuna valutazione finora
- Stratification in The Older Adult For Operative RiskDocumento24 pagineStratification in The Older Adult For Operative RiskshodhgangaNessuna valutazione finora
- CBR - OrthoticsDocumento33 pagineCBR - Orthoticsshodhganga50% (2)
- Walking Abilities of Young Adults With Cerebral Palsy After Multilevel SurgeryDocumento7 pagineWalking Abilities of Young Adults With Cerebral Palsy After Multilevel SurgeryshodhgangaNessuna valutazione finora
- Stepping Exercises Improve Muscle Strength in The Early Postoperative Phase After Total Hip ArthroplastyDocumento10 pagineStepping Exercises Improve Muscle Strength in The Early Postoperative Phase After Total Hip ArthroplastyshodhgangaNessuna valutazione finora
- Goniometry of ULDocumento55 pagineGoniometry of ULshodhgangaNessuna valutazione finora
- Bbi2421 SCL Worksheet 2Documento12 pagineBbi2421 SCL Worksheet 2Diane GadgetriesNessuna valutazione finora
- Time ManagementDocumento54 pagineTime Managementsalhum100% (3)
- Kesesuaian Anamnese Kefarmasian Oleh Apo 833182d5 PDFDocumento5 pagineKesesuaian Anamnese Kefarmasian Oleh Apo 833182d5 PDFelvinaNessuna valutazione finora
- a-EHS-I-004.3 Site Safety Plan (SSP), Rev.BDocumento43 paginea-EHS-I-004.3 Site Safety Plan (SSP), Rev.BAbdul Rozak Arrazy100% (1)
- Body Posture: A Detailed Lesson Plan in Pe and HealthDocumento11 pagineBody Posture: A Detailed Lesson Plan in Pe and HealthRelcy AnnNessuna valutazione finora
- 7 Youth Awareness - A Survey On Mobile Gaming Addiction Concerning Physical Health Performance On Young Adults in MalaysiaDocumento14 pagine7 Youth Awareness - A Survey On Mobile Gaming Addiction Concerning Physical Health Performance On Young Adults in MalaysiaEdielyn Gonzalvo GutierrezNessuna valutazione finora
- COVID-19 Cases and Deaths in South Carolina Nursing HomesDocumento3 pagineCOVID-19 Cases and Deaths in South Carolina Nursing HomesWIS Digital News Staff50% (2)
- Nurse Patient Relationship Research PaperDocumento11 pagineNurse Patient Relationship Research PaperLen ZinxNessuna valutazione finora
- Cardiff PacesDocumento26 pagineCardiff PacesIvyljn100% (2)
- 8-Material Safety Data SheetDocumento2 pagine8-Material Safety Data Sheetreadyboy89Nessuna valutazione finora
- AQA Unit 2 Sociology of Health (5) Disability: The Biomedical Approach To DisabilityDocumento10 pagineAQA Unit 2 Sociology of Health (5) Disability: The Biomedical Approach To DisabilityClean ToneNessuna valutazione finora
- Factors Affecting The Academic Performance of The Bsba Working Students in Kolehiyo NG Subic S.Y. 2018-2019Documento65 pagineFactors Affecting The Academic Performance of The Bsba Working Students in Kolehiyo NG Subic S.Y. 2018-2019Regie LuluquisinNessuna valutazione finora
- Kardex: Mental Status: Activities: Diet: Tubes: Special InfoDocumento3 pagineKardex: Mental Status: Activities: Diet: Tubes: Special InfoRyrey Abraham PacamanaNessuna valutazione finora
- Porfolio NFDN 2005Documento2 paginePorfolio NFDN 2005api-318906225100% (1)
- Test Bank For Medical Terminology For Health Professions 8th Edition by EhrlichDocumento13 pagineTest Bank For Medical Terminology For Health Professions 8th Edition by EhrlichJames Chapman100% (35)
- Ibs PDFDocumento13 pagineIbs PDFharrysudarmaNessuna valutazione finora
- Executive SummaryDocumento2 pagineExecutive SummaryFaisal RezwanNessuna valutazione finora
- Field Trip Risk AssessmentDocumento4 pagineField Trip Risk Assessmentapi-287142055100% (1)
- Art 10Documento11 pagineArt 10Maria Del Carmen MaciasNessuna valutazione finora
- FPM Advanced PainDocumento11 pagineFPM Advanced PainHisham SalamehNessuna valutazione finora
- Supervision: Aparna M Ajay Asst - Professor, College of NursingDocumento53 pagineSupervision: Aparna M Ajay Asst - Professor, College of NursingAparna Kingini100% (1)
- Procedure Checklist Chapter 23: Administering IV Push Medications Through A Running Primary IV LineDocumento2 pagineProcedure Checklist Chapter 23: Administering IV Push Medications Through A Running Primary IV LineLiezel CauilanNessuna valutazione finora
- Cold Chain Management IdeasDocumento11 pagineCold Chain Management IdeasRajat GargNessuna valutazione finora
- Final Exam in Gec 5Documento2 pagineFinal Exam in Gec 5Janine PantiNessuna valutazione finora
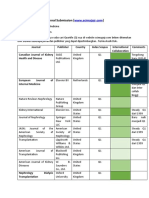
- Journal SubmissionDocumento3 pagineJournal SubmissionMaruhum Bonar MarbunNessuna valutazione finora
- Physical EducationDocumento16 paginePhysical EducationIan Jay MacaraegNessuna valutazione finora
- CBC Rice Machinery OperationDocumento10 pagineCBC Rice Machinery OperationAndrea PabalinasNessuna valutazione finora
- Impaired Skin IntegDocumento2 pagineImpaired Skin IntegMarcus Philip GonzalesNessuna valutazione finora
- Peranan Dan Tanggungjawab PPPDocumento19 paginePeranan Dan Tanggungjawab PPPAcillz M. HaizanNessuna valutazione finora
- Access Program CouponDocumento1 paginaAccess Program CouponipkwokhungNessuna valutazione finora