Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Can "Daniel's Diabetic Miracle" Naturally Heal Diabetes in As Little As 3 DaysDocumento33 pagineCan "Daniel's Diabetic Miracle" Naturally Heal Diabetes in As Little As 3 Daysaz75% (4)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Applying For Jobs Ebook Ed 1Documento41 pagineApplying For Jobs Ebook Ed 11234chocoNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Nicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFDocumento927 pagineNicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFJamie Baczewski100% (8)
- USMLE Flashcards: Anatomy - Side by SideDocumento190 pagineUSMLE Flashcards: Anatomy - Side by SideMedSchoolStuff100% (3)
- Concepts of Public HealthDocumento8 pagineConcepts of Public Healtharn0ld21Nessuna valutazione finora
- Obstructed LabourDocumento2 pagineObstructed LabourAvinash BarhateNessuna valutazione finora
- DR - Prateek ResumeDocumento1 paginaDR - Prateek ResumePrateek KumarNessuna valutazione finora
- Periodontology III MCQ For The FinalDocumento55 paginePeriodontology III MCQ For The FinalLolita A. Hicks50% (2)
- Language of PreventionDocumento9 pagineLanguage of Prevention1234chocoNessuna valutazione finora
- Congenital HypothyroidismDocumento2 pagineCongenital Hypothyroidismapi-321672273Nessuna valutazione finora
- Pokemon Theme Song 22Documento4 paginePokemon Theme Song 221234chocoNessuna valutazione finora
- Code Geass - StoriesDocumento5 pagineCode Geass - Stories1234chocoNessuna valutazione finora
- Blue Veins Sub Theme TVBDocumento4 pagineBlue Veins Sub Theme TVB1234chocoNessuna valutazione finora
- Fairy Tail - Main ThemeDocumento3 pagineFairy Tail - Main Theme1234chocoNessuna valutazione finora
- Mbs Quick Guide: JULY 2020Documento2 pagineMbs Quick Guide: JULY 20201234chocoNessuna valutazione finora
- QLD Rail Traim PDFDocumento1 paginaQLD Rail Traim PDF1234chocoNessuna valutazione finora
- Blue BirdDocumento7 pagineBlue Bird1234chocoNessuna valutazione finora
- VTE GuidelinesDocumento11 pagineVTE Guidelines1234chocoNessuna valutazione finora
- Taking A Social and Cultural HistoryDocumento3 pagineTaking A Social and Cultural History1234chocoNessuna valutazione finora
- Doctor Talk: Communication Practice Role PlaysDocumento6 pagineDoctor Talk: Communication Practice Role Plays1234chocoNessuna valutazione finora
- Osteo Infographic FinalDocumento1 paginaOsteo Infographic Final1234chocoNessuna valutazione finora
- Acute Low Back Pain Flowchart January 2017Documento1 paginaAcute Low Back Pain Flowchart January 20171234chocoNessuna valutazione finora
- Topical Steroids (Sep 19) PDFDocumento7 pagineTopical Steroids (Sep 19) PDF1234chocoNessuna valutazione finora
- Topical Steroids (Sep 19) PDFDocumento7 pagineTopical Steroids (Sep 19) PDF1234chocoNessuna valutazione finora
- Fluids ElectrolytesDocumento2 pagineFluids Electrolytes1234chocoNessuna valutazione finora
- FLOWCHART - ARC Adult Cardiorespiratory ArrestDocumento1 paginaFLOWCHART - ARC Adult Cardiorespiratory Arrest1234chocoNessuna valutazione finora
- Metro South Intern Training Form (Logan)Documento3 pagineMetro South Intern Training Form (Logan)1234chocoNessuna valutazione finora
- PBM Module1 MTP Template 0Documento2 paginePBM Module1 MTP Template 01234chocoNessuna valutazione finora
- 2016 Applicant Guide Web V2Documento83 pagine2016 Applicant Guide Web V21234chocoNessuna valutazione finora
- Managing Mental Illness in Patients From CALD Backgrounds: PsychiatryDocumento5 pagineManaging Mental Illness in Patients From CALD Backgrounds: Psychiatry1234chocoNessuna valutazione finora
- Defining and Assessing Risks To Health PDFDocumento20 pagineDefining and Assessing Risks To Health PDF1234chocoNessuna valutazione finora
- A Conceptual Framework For HealthDocumento1 paginaA Conceptual Framework For Health1234chocoNessuna valutazione finora
- Herd Immunity'' A Rough Guide PDFDocumento6 pagineHerd Immunity'' A Rough Guide PDF1234chocoNessuna valutazione finora
- The Effects of Social Networks On Disability in Older AustraliansDocumento22 pagineThe Effects of Social Networks On Disability in Older Australians1234chocoNessuna valutazione finora
- ImprovingMedAdherenceOlderAdultslyer Final 508CDocumento2 pagineImprovingMedAdherenceOlderAdultslyer Final 508CKumar PatilNessuna valutazione finora
- Clinical Contributions To Addressing The Social Determinants of HealthDocumento5 pagineClinical Contributions To Addressing The Social Determinants of Health1234chocoNessuna valutazione finora
- Prevalence of Use of Complementary/alternative Medicine: A Systematic ReviewDocumento6 paginePrevalence of Use of Complementary/alternative Medicine: A Systematic ReviewGilang Febri PratamaNessuna valutazione finora
- COVID-19 Vaccine Acceptability and Its Determinants in Mozambique: An Online SurveyDocumento10 pagineCOVID-19 Vaccine Acceptability and Its Determinants in Mozambique: An Online Surveyh3493061Nessuna valutazione finora
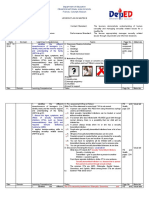
- DLL - First GradingDocumento5 pagineDLL - First GradingMeek Adan Rodriguez100% (2)
- VVND TreatmentDocumento4 pagineVVND Treatmentkarthivisu2009100% (1)
- Kizilarslanoglu 2016Documento7 pagineKizilarslanoglu 2016EviNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaIntania MairudiNessuna valutazione finora
- Safety and Efficacy of The BNT162b2 MRNA Covid-19 Vaccine Through 6 MonthsDocumento13 pagineSafety and Efficacy of The BNT162b2 MRNA Covid-19 Vaccine Through 6 MonthsChristian GaraffaNessuna valutazione finora
- Modified Diploma Logbook 2011 2012Documento109 pagineModified Diploma Logbook 2011 2012Khalid ElmasryNessuna valutazione finora
- Raw Milk For The HealthDocumento7 pagineRaw Milk For The HealthviannikkkyNessuna valutazione finora
- Hempel Vs Cydan Et Al-ComplaintDocumento34 pagineHempel Vs Cydan Et Al-Complaintforbesadmin100% (1)
- Comparison of Nursing and Medical DiagnosesDocumento14 pagineComparison of Nursing and Medical DiagnosesNeko NekoNessuna valutazione finora
- National Strategic Plan 2017-25Documento144 pagineNational Strategic Plan 2017-25SNessuna valutazione finora
- CGH:2018 09 13:maravillaDocumento3 pagineCGH:2018 09 13:maravillaRachelle MaravillaNessuna valutazione finora
- Do Not Resuscitate Orders: Among Physicians, Nurses, Patients and RelativesDocumento4 pagineDo Not Resuscitate Orders: Among Physicians, Nurses, Patients and RelativesSalman HabeebNessuna valutazione finora
- Candida Infection, Integrated Science, 4.3Documento13 pagineCandida Infection, Integrated Science, 4.3Anesia Andrews100% (1)
- Roles of Oncology Pharmacists in Korea 20140928Documento17 pagineRoles of Oncology Pharmacists in Korea 20140928adeputra25Nessuna valutazione finora
- Family Health Nursing CHN (Start Midterm)Documento4 pagineFamily Health Nursing CHN (Start Midterm)Aiza OronceNessuna valutazione finora
- Small PoxDocumento2 pagineSmall PoxTimNessuna valutazione finora
- Cinical Scenario CholelithiasisDocumento2 pagineCinical Scenario CholelithiasisSarine GonzalezNessuna valutazione finora
- Arsenic - IARC Monograph V84Documento526 pagineArsenic - IARC Monograph V84ACNessuna valutazione finora
- Industry Breakdown Episode 2: "Pharmaceuticals"Documento7 pagineIndustry Breakdown Episode 2: "Pharmaceuticals"KAVYA GOYAL PGP 2021-23 BatchNessuna valutazione finora
- CARE ScriptDocumento3 pagineCARE ScriptJay SteeleNessuna valutazione finora
- Sample Leave Restriction LetterDocumento3 pagineSample Leave Restriction LetterGayathriNessuna valutazione finora