Potrebbero piacerti anche
- Physiology for General Surgical Sciences Examination (GSSE)Da EverandPhysiology for General Surgical Sciences Examination (GSSE)S. Ali MirjaliliNessuna valutazione finora
- Drugs Used in Disorders of CoagulationDocumento60 pagineDrugs Used in Disorders of CoagulationTwinkle MazaredoNessuna valutazione finora
- Blood Coagulation and FibrinolysisDocumento63 pagineBlood Coagulation and FibrinolysisNora AboshanadyNessuna valutazione finora
- Anticoagulation Guidelines JMDocumento32 pagineAnticoagulation Guidelines JMMichael HuntNessuna valutazione finora
- Fibrinolitiktrombolitik, Antikoagulan Dan AntiplateletDocumento31 pagineFibrinolitiktrombolitik, Antikoagulan Dan AntiplateletAnggra OlgabellaNessuna valutazione finora
- Pos NoacDocumento40 paginePos NoacSanjeev Harry Budhooram100% (1)
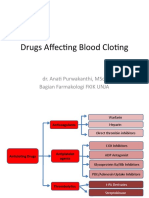
- Drugs Affecting Blood Cloting 2019Documento39 pagineDrugs Affecting Blood Cloting 2019Mutiara RizkiNessuna valutazione finora
- Antiplatelet DrugsDocumento19 pagineAntiplatelet Drugsngan321Nessuna valutazione finora
- Nsaids DrugsDocumento2 pagineNsaids DrugsIrene Zae MwandotoNessuna valutazione finora
- Drugs Use in HemostasisDocumento47 pagineDrugs Use in HemostasiskadibhaNessuna valutazione finora
- Anti-Coagulants, Anti-Platelets, FibrinolyticsDocumento1 paginaAnti-Coagulants, Anti-Platelets, FibrinolyticsGerardLum100% (1)
- Principles of An-Tiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyDocumento36 paginePrinciples of An-Tiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyAbby LiewNessuna valutazione finora
- 3 Blood Coagulation DrugsDocumento20 pagine3 Blood Coagulation DrugsAudrey Beatrice ReyesNessuna valutazione finora
- Anti CoagulantsDocumento25 pagineAnti Coagulantsshoaib106muhammadNessuna valutazione finora
- Year 1 Drugs List (Medicine)Documento33 pagineYear 1 Drugs List (Medicine)Anonymous IwWT90VyNessuna valutazione finora
- Have Half-Lives in The Range 2 - 6 H. Lovenox Is 4.5 Hours. The Anticoagulant Effect ofDocumento37 pagineHave Half-Lives in The Range 2 - 6 H. Lovenox Is 4.5 Hours. The Anticoagulant Effect ofkellixgNessuna valutazione finora
- Anticoagulants 2019Documento11 pagineAnticoagulants 2019Srijan VermaNessuna valutazione finora
- Principles of Antiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyDocumento36 paginePrinciples of Antiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyAbby Liew100% (1)
- StreptokinaseDocumento8 pagineStreptokinaseemman_abzNessuna valutazione finora
- Coagulation Modifier Drugs: Lilley Reading and Workbook, Chap 27Documento38 pagineCoagulation Modifier Drugs: Lilley Reading and Workbook, Chap 27Peter Angelo GeleraNessuna valutazione finora
- Cardiology Pharmacology Review: Dhiren Patel, Pharmd, CdeDocumento74 pagineCardiology Pharmacology Review: Dhiren Patel, Pharmd, Cdeshannon_marrero_1Nessuna valutazione finora
- Assess Extrinsic Pathway (Tissue Factor Pathway) Prothrombin Time / PT Test / INRDocumento3 pagineAssess Extrinsic Pathway (Tissue Factor Pathway) Prothrombin Time / PT Test / INRKristin DouglasNessuna valutazione finora
- Anti Clotting, Fibrinolytic, Tests For CoagulationDocumento70 pagineAnti Clotting, Fibrinolytic, Tests For CoagulationDr.Gomathi sivakumarNessuna valutazione finora
- AntidotesDocumento2 pagineAntidotesYemaya84Nessuna valutazione finora
- MedSurg Medications & TablesDocumento71 pagineMedSurg Medications & TablesSarah PlunkettNessuna valutazione finora
- Drugs For GI DisordersDocumento5 pagineDrugs For GI DisordersAalap ShahNessuna valutazione finora
- Drugs Used in Disorders of CoagulationDocumento61 pagineDrugs Used in Disorders of CoagulationDUEÑAS, MARIELNessuna valutazione finora
- Parasympathetic Nervous System: Uptake of CholineDocumento16 pagineParasympathetic Nervous System: Uptake of Cholinegksah711Nessuna valutazione finora
- Drugs For Coagulation Disorders 2023Documento26 pagineDrugs For Coagulation Disorders 2023aguilarjanicaNessuna valutazione finora
- Acute Gastric Mucosal LesionDocumento19 pagineAcute Gastric Mucosal LesionYan_ChiiNessuna valutazione finora
- 14 BloodDocumento32 pagine14 Bloodنور الإسلامNessuna valutazione finora
- Pharmacology: Teratogenic CarcinogenicDocumento13 paginePharmacology: Teratogenic CarcinogenicSherlock HolmesNessuna valutazione finora
- Anticoagulants DrugsDocumento6 pagineAnticoagulants DrugsHusam Al-OdatNessuna valutazione finora
- Anticoagulants: (Parenteral)Documento38 pagineAnticoagulants: (Parenteral)susan2johnson-501300Nessuna valutazione finora
- Pharma DR - Hussein Drugs Effecting Hemostasis Lec 1Documento31 paginePharma DR - Hussein Drugs Effecting Hemostasis Lec 1rkh647m7szNessuna valutazione finora
- Obat Sistem HematologiDocumento21 pagineObat Sistem HematologiSuryana AdityaNessuna valutazione finora
- Anticoagulants: Dr. Hassan Mohamed EnowDocumento37 pagineAnticoagulants: Dr. Hassan Mohamed EnowFatimaNessuna valutazione finora
- AnticoagulantsDocumento3 pagineAnticoagulantsDarNessuna valutazione finora
- Current Cardiovascular Therapy Pharmacological-229-246Documento18 pagineCurrent Cardiovascular Therapy Pharmacological-229-246Yulian 53Nessuna valutazione finora
- Thrombolytics, Anticoags, Antiplatelets PDFDocumento21 pagineThrombolytics, Anticoags, Antiplatelets PDFrachelkdoNessuna valutazione finora
- M MMM MMDocumento10 pagineM MMM MMMustafa Al-Nua'aimyNessuna valutazione finora
- Thrombolytics & Anti Platelet DrugsDocumento38 pagineThrombolytics & Anti Platelet DrugsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Coagulants and AnticoagulantsDocumento5 pagineCoagulants and AnticoagulantsMuhammad AsifNessuna valutazione finora
- Anticoagulation Reversal AgentsDocumento3 pagineAnticoagulation Reversal AgentsElaine Yves JulineNessuna valutazione finora
- Heparin Warfarin Sodium (Coumadin)Documento5 pagineHeparin Warfarin Sodium (Coumadin)أبوأحمد الحكيمNessuna valutazione finora
- Pharmacology RCR1 - CardioDocumento8 paginePharmacology RCR1 - CardioeamcrawleyNessuna valutazione finora
- Drugs Affecting Coagulation ObjectivesDocumento14 pagineDrugs Affecting Coagulation ObjectiveslouradelNessuna valutazione finora
- Drug StudyDocumento2 pagineDrug StudymatthewchadNessuna valutazione finora
- Pharmacology and Toxicology - Anticoagulants - Medical LibraryDocumento8 paginePharmacology and Toxicology - Anticoagulants - Medical Libraryjean PiedraNessuna valutazione finora
- 1120314晨會 Miller Ch50. Patient Blood Management CoagulationDocumento56 pagine1120314晨會 Miller Ch50. Patient Blood Management Coagulationw8412358Nessuna valutazione finora
- 2015 Anticoagulants and AntiplateletsDocumento53 pagine2015 Anticoagulants and AntiplateletsAldi SadegaNessuna valutazione finora
- Drugs Med-SurgTest 3Documento6 pagineDrugs Med-SurgTest 3Sarah PlunkettNessuna valutazione finora
- ANTI PlateletDocumento3 pagineANTI PlateletZanga MusakuziNessuna valutazione finora
- Application of Pharmacognosy in Clinical Practice - Group 5Documento26 pagineApplication of Pharmacognosy in Clinical Practice - Group 5Alyssa Nicole PadillaNessuna valutazione finora
- Hematology FA - 1Documento78 pagineHematology FA - 1JaankiNessuna valutazione finora
- Pharmacology MendozaDocumento27 paginePharmacology MendozaBlaine ManiegoNessuna valutazione finora
- Drugs Related To ClottingDocumento23 pagineDrugs Related To ClottingBig PigNessuna valutazione finora
- Anticoagulants May BeDocumento5 pagineAnticoagulants May BeAmmar magdyNessuna valutazione finora
- New Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011Documento55 pagineNew Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011andresrgomezNessuna valutazione finora
- Disseminated Intravascular CoagulationDocumento2 pagineDisseminated Intravascular CoagulationKeserovic AdmirNessuna valutazione finora
- Chronic Leg Ulcer Post Phlebitic Limb Syndrome: Homan's Sign - Forceful Dorsiflexion of Foot Will Cause Pain in CalfDocumento4 pagineChronic Leg Ulcer Post Phlebitic Limb Syndrome: Homan's Sign - Forceful Dorsiflexion of Foot Will Cause Pain in CalfKeserovic AdmirNessuna valutazione finora
- Biochemical Changes of Diabetes MellitusDocumento5 pagineBiochemical Changes of Diabetes MellitusKeserovic AdmirNessuna valutazione finora
- Acutescrotum 141125014842 Conversion Gate01Documento18 pagineAcutescrotum 141125014842 Conversion Gate01Keserovic AdmirNessuna valutazione finora
- Penicill IN: Praksh Dhakal Public Health Microbiology Tribhuvan UniversityDocumento22 paginePenicill IN: Praksh Dhakal Public Health Microbiology Tribhuvan UniversityKeserovic AdmirNessuna valutazione finora
- Urology Resident Handbook3380 PDFDocumento65 pagineUrology Resident Handbook3380 PDFKeserovic AdmirNessuna valutazione finora
- Examination of Thyroid GlandDocumento2 pagineExamination of Thyroid GlandKeserovic Admir100% (1)
- Renal Osteodystrophy: ( Glomerular Filtration)Documento4 pagineRenal Osteodystrophy: ( Glomerular Filtration)Keserovic AdmirNessuna valutazione finora
- Genitourinary Emergency: Prof. Dr. Mostafa Sakr Genitourinary SurgeryDocumento83 pagineGenitourinary Emergency: Prof. Dr. Mostafa Sakr Genitourinary SurgeryKeserovic AdmirNessuna valutazione finora
- Urinary Tract Infections in ChildrenDocumento2 pagineUrinary Tract Infections in ChildrenKeserovic AdmirNessuna valutazione finora
- Diabetes IN Pregnanc Y: Presenter: DR Leong Yuh Yang (MD Ukm) Supervisor: DR Noraza AzmeeraDocumento45 pagineDiabetes IN Pregnanc Y: Presenter: DR Leong Yuh Yang (MD Ukm) Supervisor: DR Noraza AzmeeraKeserovic AdmirNessuna valutazione finora
- HaematinicsDocumento2 pagineHaematinicsGerardLum100% (2)
- 161106115611Documento3 pagine161106115611Keserovic AdmirNessuna valutazione finora
- Lymph Node Pathology PDFDocumento4 pagineLymph Node Pathology PDFKeserovic AdmirNessuna valutazione finora
- Antimalarials - Are They Effective and Safe in Rheumatic DiseasesDocumento10 pagineAntimalarials - Are They Effective and Safe in Rheumatic DiseasesYahya RizkiNessuna valutazione finora
- Routine For 8th Sem 2017Documento5 pagineRoutine For 8th Sem 2017Tanbir MukherjeeNessuna valutazione finora
- Master Formula CardDocumento7 pagineMaster Formula CardTrilochan Ayurveda100% (1)
- Chemical Company Brochure PDF Anmol Chemicals Pvt. Ltd. Company ProfileDocumento21 pagineChemical Company Brochure PDF Anmol Chemicals Pvt. Ltd. Company ProfileAnmol ChemicalsNessuna valutazione finora
- Herbal Property Dictionary SampleDocumento27 pagineHerbal Property Dictionary Sampledarkllight100% (3)
- Clientes Farmovet 16-11Documento4 pagineClientes Farmovet 16-11Christian Alejandro BarretoNessuna valutazione finora
- FormulationsDocumento8 pagineFormulationsVaishali Chavan-YewaleNessuna valutazione finora
- Quaalude PDFDocumento8 pagineQuaalude PDFtom100% (1)
- Evaluation ToolDocumento4 pagineEvaluation ToolCarlos TorresNessuna valutazione finora
- Coversam 4mg/5mg Tablets Coversam 4mg/10mg Tablets Coversam 8mg/5mg Tablets Coversam 8mg/10mg TabletsDocumento2 pagineCoversam 4mg/5mg Tablets Coversam 4mg/10mg Tablets Coversam 8mg/5mg Tablets Coversam 8mg/10mg TabletsRaheel Neo AhmadNessuna valutazione finora
- Anti Anginal DrugsDocumento1 paginaAnti Anginal DrugsHatem AbouelnasrNessuna valutazione finora
- Ranitidine NeomedDocumento5 pagineRanitidine NeomedMarsyaNessuna valutazione finora
- Photo StabilityDocumento11 paginePhoto StabilityHaroon RasheedNessuna valutazione finora
- Safety Aspects of AyurvedaDocumento12 pagineSafety Aspects of AyurvedaRajnish PandeyNessuna valutazione finora
- Dispatches From The War Zone of EnvironmentalDocumento336 pagineDispatches From The War Zone of EnvironmentalwxcvbnnbvcxwNessuna valutazione finora
- Produttori AzitroDocumento10 pagineProduttori AzitroMario MicciarelliNessuna valutazione finora
- CBD Clinic Massage Oil 12oz 11.7.18Documento1 paginaCBD Clinic Massage Oil 12oz 11.7.18Jose MaldonadoNessuna valutazione finora
- Chronic Renal FailureDocumento40 pagineChronic Renal FailureSarumathy PrabakaranNessuna valutazione finora
- Paracetamol 1Documento4 pagineParacetamol 1Jeremiah Justus MNessuna valutazione finora
- Farmakoterapi Pada LansiaDocumento29 pagineFarmakoterapi Pada LansiaPuterinugraha Wanca ApatyaNessuna valutazione finora
- 228-237 CSR Pharma PDFDocumento10 pagine228-237 CSR Pharma PDFSavia Mendes E DsouzaNessuna valutazione finora
- History of AnesthesiologyDocumento2 pagineHistory of AnesthesiologyCms CSUNessuna valutazione finora
- Visual Infusion Phlebitis ScoreDocumento2 pagineVisual Infusion Phlebitis ScoreAnggita Agustina100% (1)
- Meds For Print 2Documento9 pagineMeds For Print 2Alex SibalNessuna valutazione finora
- In Vitro, Sucralfate Adsorbs Bile SaltsDocumento5 pagineIn Vitro, Sucralfate Adsorbs Bile SaltsZarbakht AliNessuna valutazione finora
- Medikolegal Pengobatan Untuk Diri Sendiri (Swamedikasi) Sebagai Upaya Menyembuhkan PenyakitDocumento8 pagineMedikolegal Pengobatan Untuk Diri Sendiri (Swamedikasi) Sebagai Upaya Menyembuhkan PenyakitMiftahul JannahNessuna valutazione finora
- Antidepressants For The Treatment of InsomniaDocumento8 pagineAntidepressants For The Treatment of Insomniaapi-19853437Nessuna valutazione finora
- PharmaBiotech Flyer 105x210mm Low 140312Documento16 paginePharmaBiotech Flyer 105x210mm Low 140312Yaqoob AliNessuna valutazione finora
- 2000, Antonow J. Medication Error Reporting PediatriaDocumento7 pagine2000, Antonow J. Medication Error Reporting PediatriaFilipa Salvador SalvadorNessuna valutazione finora