Potrebbero piacerti anche
- Case Study-Gastric CancerDocumento19 pagineCase Study-Gastric Cancerbhelskie100% (2)
- Colon Cancer Case StudyDocumento18 pagineColon Cancer Case Studyapi-271062060100% (2)
- Cancer Case StudyDocumento23 pagineCancer Case StudyMeynard AndresNessuna valutazione finora
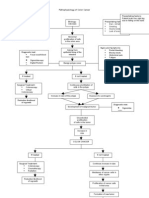
- Pathophysiology For Colorectal CancerDocumento12 paginePathophysiology For Colorectal CancerRosemarie Carpio100% (6)
- A Case Study On Rectal AdenocarcinomaDocumento62 pagineA Case Study On Rectal AdenocarcinomaEyySiEffVee100% (1)
- Colon CancerDocumento25 pagineColon CancerKylie Golindang100% (1)
- Cancer Case StudyDocumento23 pagineCancer Case StudyJaymica Laggui DacquilNessuna valutazione finora
- A Case Study On Colon MassDocumento29 pagineA Case Study On Colon MassDahlia D. SuelloNessuna valutazione finora
- Pathophysiology of Breast CancerDocumento3 paginePathophysiology of Breast Cancerpauline mangadaNessuna valutazione finora
- Casestudy Gastric CarcinomaDocumento56 pagineCasestudy Gastric CarcinomaMJ Amarillo92% (12)
- Colorectal CancerDocumento8 pagineColorectal Cancerjorgeacct100% (3)
- Tribhuwan University Institute of Medicine Nepalgunj Nursing Campus Bns ProgrammeDocumento76 pagineTribhuwan University Institute of Medicine Nepalgunj Nursing Campus Bns Programmeone twoNessuna valutazione finora
- Case Study Breast CancerDocumento26 pagineCase Study Breast CancerhansNessuna valutazione finora
- Colon Ca Case Study For Ring BoundDocumento66 pagineColon Ca Case Study For Ring BoundMary EnsomoNessuna valutazione finora
- Cancer Case StudyDocumento15 pagineCancer Case StudyRobin HaliliNessuna valutazione finora
- Cancer of The ColonDocumento8 pagineCancer of The Colonnot your medz duranNessuna valutazione finora
- Case Study Colorectal CancerDocumento23 pagineCase Study Colorectal CancerLeogalvez BedanoNessuna valutazione finora
- Colorectal CancerDocumento50 pagineColorectal CancerHans Chester Rirao Capinding100% (2)
- 2 Acute CholecystitisDocumento21 pagine2 Acute CholecystitisEtteh MaryNessuna valutazione finora
- A Case Study On Breast Cancer (2003)Documento58 pagineA Case Study On Breast Cancer (2003)Katty Rine100% (6)
- AML Case StudyDocumento66 pagineAML Case StudyNoel Christian PeraltaNessuna valutazione finora
- CholelithiasisDocumento5 pagineCholelithiasisrgflores1979100% (2)
- Case Study-Breast CADocumento11 pagineCase Study-Breast CAJoanna Cabildo83% (6)
- Pa Tho Physiology of Colon CancerDocumento2 paginePa Tho Physiology of Colon Cancernick_nock0893% (14)
- Acute PancreatitisDocumento40 pagineAcute Pancreatitisjpacheco39100% (4)
- Lung Ca Case Presentation PDFDocumento28 pagineLung Ca Case Presentation PDFapi-276417422100% (2)
- Final CholelithiasisDocumento36 pagineFinal CholelithiasisRalph Pelegrino100% (2)
- Anatomy and Physiology of Peptic UlcerDocumento16 pagineAnatomy and Physiology of Peptic UlcerDrNarayan KR100% (8)
- Ovarian New GrowthDocumento7 pagineOvarian New GrowthRegiena Tamargo100% (1)
- Case Study Breast CancerDocumento25 pagineCase Study Breast CancerRalph Neil Manlutac100% (1)
- Liver CancerDocumento1 paginaLiver CancerTarantado67% (3)
- Breasy Cancer (Ductal Carcinoma) Stage 4 With Bone Metastasis PathophysiologyDocumento7 pagineBreasy Cancer (Ductal Carcinoma) Stage 4 With Bone Metastasis Pathophysiologyjudssalangsang100% (2)
- Breast CancerDocumento53 pagineBreast CancerChristine Karen Ang Suarez100% (3)
- Lung CancerDocumento25 pagineLung CancerCarla Mae Guillermo NavarroNessuna valutazione finora
- Case StudyDocumento33 pagineCase StudySarah GatuzNessuna valutazione finora
- Cancer Pathophysiology FinalDocumento3 pagineCancer Pathophysiology FinalAngelique Ramos Pascua100% (1)
- Case Study 1 0 - Pancreatic Cancer FinalDocumento23 pagineCase Study 1 0 - Pancreatic Cancer Finalapi-270737306Nessuna valutazione finora
- Acute and Chronic GastritisDocumento17 pagineAcute and Chronic GastritisIndah Nur PratiwiNessuna valutazione finora
- Lung CancerDocumento4 pagineLung CancerKrizia TepootNessuna valutazione finora
- Diagram of Pathophysiology CancerDocumento5 pagineDiagram of Pathophysiology CancerKristaMaeC.Lazo0% (3)
- Colon CancerDocumento13 pagineColon Cancerlendiibanez100% (1)
- In Partial Fulfillment of Our Requirements IN Related Learning ExperienceDocumento32 pagineIn Partial Fulfillment of Our Requirements IN Related Learning Experiencedolly joy100% (4)
- CP On Breast CancerDocumento100 pagineCP On Breast Cancerkathy50% (2)
- Pathophysiology of Colon Cancer 1Documento3 paginePathophysiology of Colon Cancer 1Katherine Clarisse Carvajal Lavarias100% (1)
- PancreatitisDocumento12 paginePancreatitisjhodane100% (4)
- Liver CancerDocumento44 pagineLiver CancerEjay Jacob Ricamara50% (2)
- Breast CancerDocumento11 pagineBreast CancerRock'nRoll Buddies100% (2)
- Nursing Care Plan of Colorectal PatientDocumento16 pagineNursing Care Plan of Colorectal PatientIkenna Okpala100% (2)
- Breast Cancer 1Documento194 pagineBreast Cancer 1Connie SianiparNessuna valutazione finora
- DIOLA-AAN202 Oncology Coursework v02 PDFDocumento88 pagineDIOLA-AAN202 Oncology Coursework v02 PDFLucian Caelum100% (1)
- Cholecystitis With CholelithiasisDocumento20 pagineCholecystitis With CholelithiasisrhyanneNessuna valutazione finora
- Case Presentation Lung CA FinalDocumento102 pagineCase Presentation Lung CA FinalMinerva Joan Escobido50% (2)
- Araullo University FinalDocumento19 pagineAraullo University FinalManzano JenecaNessuna valutazione finora
- Pancreatic CancerDocumento15 paginePancreatic CancerMutiana Muspita JeliNessuna valutazione finora
- Case PresDocumento18 pagineCase Prestiban_07Nessuna valutazione finora
- Ibn-Sina Nursing and Midwifery Collage Case Study "Nursing Management"Documento14 pagineIbn-Sina Nursing and Midwifery Collage Case Study "Nursing Management"مالك مناصرةNessuna valutazione finora
- Case StudyDocumento17 pagineCase StudyEarl Viray JulaoNessuna valutazione finora
- Case Study - OTITIS MEDIADocumento9 pagineCase Study - OTITIS MEDIAHasing Amado100% (1)
- Farah Cwu Gynae EditDocumento16 pagineFarah Cwu Gynae EditfarahNessuna valutazione finora
- Pathophy EsrdDocumento4 paginePathophy EsrdVecky TolentinoNessuna valutazione finora
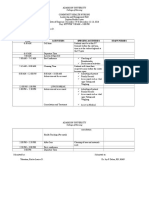
- Day 5 Time Activities Specific Activities Staff Nurses: College of NursingDocumento2 pagineDay 5 Time Activities Specific Activities Staff Nurses: College of NursingVecky TolentinoNessuna valutazione finora
- Management Plan: Head Nurse: Tolentino, Ericka Louise Area: FEU-NRMFDocumento2 pagineManagement Plan: Head Nurse: Tolentino, Ericka Louise Area: FEU-NRMFVecky TolentinoNessuna valutazione finora
- Summary of GradesDocumento1 paginaSummary of GradesVecky TolentinoNessuna valutazione finora
- ESRD Lab Test, Drug Study and NCPDocumento3 pagineESRD Lab Test, Drug Study and NCPVecky TolentinoNessuna valutazione finora
- ESRDDocumento37 pagineESRDVecky TolentinoNessuna valutazione finora
- What Is End-Stage Renal Disease (ESRD) ?Documento2 pagineWhat Is End-Stage Renal Disease (ESRD) ?Vecky TolentinoNessuna valutazione finora
- FliersDocumento2 pagineFliersVecky TolentinoNessuna valutazione finora
- ESRDDocumento37 pagineESRDVecky TolentinoNessuna valutazione finora
- What Is End-Stage Renal Disease (ESRD) ?Documento2 pagineWhat Is End-Stage Renal Disease (ESRD) ?Vecky TolentinoNessuna valutazione finora
- Teaching Plan Hand WashingDocumento4 pagineTeaching Plan Hand WashingVecky Tolentino50% (2)
- Case Study Post Stroke SeizuresDocumento12 pagineCase Study Post Stroke SeizuresVecky TolentinoNessuna valutazione finora
- Discharge Plan Post SeizureDocumento2 pagineDischarge Plan Post SeizureVecky TolentinoNessuna valutazione finora
- ESRD Lab Test, Drug Study and NCPDocumento3 pagineESRD Lab Test, Drug Study and NCPVecky TolentinoNessuna valutazione finora
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocumento2 pagineAssessment Diagnosis Planning Intervention Rationale EvaluationVecky TolentinoNessuna valutazione finora
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocumento2 pagineAssessment Diagnosis Planning Intervention Rationale EvaluationVecky TolentinoNessuna valutazione finora
- FliersDocumento2 pagineFliersVecky TolentinoNessuna valutazione finora
- Viii. Nursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationDocumento6 pagineViii. Nursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationVecky TolentinoNessuna valutazione finora
- Drug StudyDocumento41 pagineDrug StudyVecky TolentinoNessuna valutazione finora
- (Methods in Molecular Biology 912) Jacques Cohen, Don Rieger (Auth.), Gary D. Smith, Jason E. Swain, Thomas B. Pool (Eds.) - Embryo Culture - Methods and Protocols-Humana Press (2012) PDFDocumento432 pagine(Methods in Molecular Biology 912) Jacques Cohen, Don Rieger (Auth.), Gary D. Smith, Jason E. Swain, Thomas B. Pool (Eds.) - Embryo Culture - Methods and Protocols-Humana Press (2012) PDFNkimsearNessuna valutazione finora
- START Triage Training PresentationDocumento85 pagineSTART Triage Training PresentationAnita Amanda100% (1)
- Reviewer 18 4 BPPK MCQDocumento5 pagineReviewer 18 4 BPPK MCQBio Data50% (2)
- 5CRMSDocumento2 pagine5CRMSpandoraelitesNessuna valutazione finora
- How Cells Harvest Chemical EnergyDocumento75 pagineHow Cells Harvest Chemical EnergylinNessuna valutazione finora
- Dr. Vijetha Shenoy Belle Associate Professor & In-Charge Clinical Biochemistry Laboratory Department of Biochemistry KMC ManipalDocumento53 pagineDr. Vijetha Shenoy Belle Associate Professor & In-Charge Clinical Biochemistry Laboratory Department of Biochemistry KMC ManipalKavya GaneshNessuna valutazione finora
- Mitsunori M, Kagayaki K, Satoshi Y, Akihiro H, Naokazu H, Ken T, Hideki A, and Takatoshi SDocumento14 pagineMitsunori M, Kagayaki K, Satoshi Y, Akihiro H, Naokazu H, Ken T, Hideki A, and Takatoshi SJasper CubiasNessuna valutazione finora
- Jawahar Navoday Vidhyalay Practice Question Paper: HKKX VaxzsthDocumento23 pagineJawahar Navoday Vidhyalay Practice Question Paper: HKKX VaxzsthSantpa TechnologiesNessuna valutazione finora
- Agriculture& Horticulture Conference BrochureDocumento6 pagineAgriculture& Horticulture Conference BrochureAgriculture conferenceNessuna valutazione finora
- A Single 10-Min Bout of Cold-Water Immersion Therapy After Strenuous Plyometric Exercise Has NoDocumento6 pagineA Single 10-Min Bout of Cold-Water Immersion Therapy After Strenuous Plyometric Exercise Has NoUmi RasyidahNessuna valutazione finora
- (Jagaran Josh) Science PDFDocumento136 pagine(Jagaran Josh) Science PDFPiyush KumarNessuna valutazione finora
- Survival at Sea For Mariners, Aviators PDFDocumento178 pagineSurvival at Sea For Mariners, Aviators PDFTrịnh Minh Khoa100% (1)
- Pseudo ExfoliationDocumento6 paginePseudo ExfoliationvannyanoyNessuna valutazione finora
- Neurovascular Holding PointsDocumento8 pagineNeurovascular Holding PointsAlexandru Baciu100% (1)
- An Introduction To Anatomy and Physiology MidwiferyDocumento108 pagineAn Introduction To Anatomy and Physiology MidwiferyGayuh Kartika100% (3)
- Facial Nerve MCQDocumento4 pagineFacial Nerve MCQIqbal Syed100% (1)
- CropSci101 Module 3Documento11 pagineCropSci101 Module 3Jetro Neil GapasinNessuna valutazione finora
- BrodmannDocumento2 pagineBrodmannEdelleMojicaDafilmotoNessuna valutazione finora
- Prosthodontics Lec 4 PDFDocumento11 pagineProsthodontics Lec 4 PDFHassan QazaniNessuna valutazione finora
- Voice Disorder 2011 PDFDocumento6 pagineVoice Disorder 2011 PDFfaidgustisyarifNessuna valutazione finora
- WBI11 01 Que 20220108Documento28 pagineWBI11 01 Que 20220108Hammodshan 7Nessuna valutazione finora
- Week 6 Facilitator Copy Week 06 Renal Failure PDFDocumento7 pagineWeek 6 Facilitator Copy Week 06 Renal Failure PDFoxyc0n999Nessuna valutazione finora
- ABC Model and Floral Evolution: ReviewDocumento7 pagineABC Model and Floral Evolution: ReviewHairunisa FebrianiNessuna valutazione finora
- Respiration (Multiple Choice) QP SolvedDocumento9 pagineRespiration (Multiple Choice) QP SolvedRiddhima ShahNessuna valutazione finora
- Abbot, Diabetes ManagementDocumento1 paginaAbbot, Diabetes ManagementMelissa Grace DizonNessuna valutazione finora
- The Scarecrow Queen (Excerpt)Documento36 pagineThe Scarecrow Queen (Excerpt)I Read YA50% (2)
- Impression Materials For Partial DentureDocumento40 pagineImpression Materials For Partial Dentureyunie0959Nessuna valutazione finora
- Assessing Thorax and LungsDocumento46 pagineAssessing Thorax and LungsmyfilesNessuna valutazione finora
- Acoustic Reflex Threshold (ART) Patterns: An Interpretation Guide For Students and Supervisors: Course Material and Exam Questions Course MaterialDocumento17 pagineAcoustic Reflex Threshold (ART) Patterns: An Interpretation Guide For Students and Supervisors: Course Material and Exam Questions Course Materialn_almagroNessuna valutazione finora