Potrebbero piacerti anche
- Principles of Cancer Biology 1st EditionDocumento57 paginePrinciples of Cancer Biology 1st Editiondarren.barnett949100% (44)
- Case Study AllDocumento22 pagineCase Study AllGeraldine Gallaron - CasipongNessuna valutazione finora
- Key chemotherapy drugs and their mechanismsDocumento7 pagineKey chemotherapy drugs and their mechanismsNoelani-Mei AscioNessuna valutazione finora
- Hematology & Oncology - Passmedicine 2012Documento64 pagineHematology & Oncology - Passmedicine 2012dheajst100% (1)
- Pharmacology - CANCER FinalDocumento18 paginePharmacology - CANCER FinalCarol NavidadNessuna valutazione finora
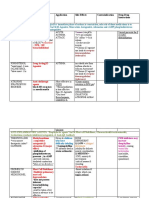
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocumento3 pagineDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinNessuna valutazione finora
- Blood Administration: NRS 108 Essec County CollegeDocumento22 pagineBlood Administration: NRS 108 Essec County CollegeDiah Puspita RiniNessuna valutazione finora
- HaemoglobinDocumento47 pagineHaemoglobinPreethi AbhilashNessuna valutazione finora
- Interpretation of Liver Enzyme Tests - A Rapid GuideDocumento3 pagineInterpretation of Liver Enzyme Tests - A Rapid Guidesserggios100% (2)
- Fibroids ADocumento242 pagineFibroids Anautilus81100% (1)
- Fast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsDa EverandFast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsNessuna valutazione finora
- Hematology Review 2021-2Documento142 pagineHematology Review 2021-2Maram AbdullahNessuna valutazione finora
- HRSDocumento63 pagineHRSPriya KalariaNessuna valutazione finora
- Fluid Resuscitation and Organ Perfusion EvaluationDocumento66 pagineFluid Resuscitation and Organ Perfusion EvaluationDewiRatnasariNessuna valutazione finora
- Bone Marrow TransplantationDocumento21 pagineBone Marrow TransplantationMorrison George100% (1)
- ALL Case PresentationDocumento43 pagineALL Case PresentationMonica MoralesNessuna valutazione finora
- Stem Cell TransplantationDocumento13 pagineStem Cell TransplantationMylls MondejarNessuna valutazione finora
- Step 2 CK Review - HematologyDocumento18 pagineStep 2 CK Review - Hematologyrsmd1986Nessuna valutazione finora
- 3 Bone Marrow ExaminationDocumento105 pagine3 Bone Marrow ExaminationShourav SarkarNessuna valutazione finora
- Clinical Presentation, Pathologic Features, Diagnosis, and Differential Diagnosis of Chronic Lymphocytic Leukemia - UpToDateDocumento23 pagineClinical Presentation, Pathologic Features, Diagnosis, and Differential Diagnosis of Chronic Lymphocytic Leukemia - UpToDateJosé Martínez100% (1)
- Cancer ChemotherapyDocumento9 pagineCancer ChemotherapyJennicaNessuna valutazione finora
- Diabetic Emergencies Case StudiesDocumento32 pagineDiabetic Emergencies Case StudiesLamria Maloni Siahaan0% (1)
- Guidelines in ChemotherapyDocumento36 pagineGuidelines in ChemotherapyIndonesian Journal of Cancer100% (1)
- Hematology MCQSDocumento36 pagineHematology MCQSLorelie ChenNessuna valutazione finora
- What Is A Bone Marrow Transplant?Documento4 pagineWhat Is A Bone Marrow Transplant?Krisna AgustiniNessuna valutazione finora
- What Is HyperlipidemiaDocumento9 pagineWhat Is Hyperlipidemiaichanara100% (2)
- Bone Marrow TransplantDocumento8 pagineBone Marrow TransplantPSRI hospitalNessuna valutazione finora
- Managing Hyperleukocytosis in Acute LeukemiaDocumento10 pagineManaging Hyperleukocytosis in Acute LeukemiaNaty AlvarezNessuna valutazione finora
- UrosepsisDocumento22 pagineUrosepsisWita Ferani KartikaNessuna valutazione finora
- Orientation To Blood Bank 2Documento24 pagineOrientation To Blood Bank 2Darshita SharmaNessuna valutazione finora
- 2023.PharmacologyLab - Trans14.CancerChemotherapyPart1 2Documento5 pagine2023.PharmacologyLab - Trans14.CancerChemotherapyPart1 2Lloyd LinNessuna valutazione finora
- LSM4225-1 CytogeneticsDocumento63 pagineLSM4225-1 CytogeneticseveNessuna valutazione finora
- Hematological Diseases and Anemia ClassificationDocumento6 pagineHematological Diseases and Anemia ClassificationBhavya agarwalNessuna valutazione finora
- Acute Myeloid Leukemia in Children 2016Documento10 pagineAcute Myeloid Leukemia in Children 2016Jorge Eduardo Espinoza RiosNessuna valutazione finora
- Acute Lymphoblastic LeukemiaDocumento7 pagineAcute Lymphoblastic LeukemiaSahara EffendyNessuna valutazione finora
- Acute Lymphocytic LeukemiaDocumento7 pagineAcute Lymphocytic LeukemiaKim Enrico JumarangNessuna valutazione finora
- Empirical Treatment of Sepsis in AdultsDocumento11 pagineEmpirical Treatment of Sepsis in AdultsMarnia SulfianaNessuna valutazione finora
- Immune Thrombocytopenic Purpura PDFDocumento12 pagineImmune Thrombocytopenic Purpura PDFAlvin PratamaNessuna valutazione finora
- Relapsed Refractory AMLDocumento114 pagineRelapsed Refractory AMLKishoreChandraKoradaNessuna valutazione finora
- Understanding Thalassemia: Causes, Symptoms and TreatmentDocumento19 pagineUnderstanding Thalassemia: Causes, Symptoms and TreatmentJayricDepalobosNessuna valutazione finora
- Identify CVD Risk in the Office with Framingham & Non-Fasting TestsDocumento28 pagineIdentify CVD Risk in the Office with Framingham & Non-Fasting TestsJuwanto Wakimin100% (1)
- Emergency Department Evaluation Back PainDocumento29 pagineEmergency Department Evaluation Back PainRodolfo GorveñaNessuna valutazione finora
- Anemia in ChildrenDocumento9 pagineAnemia in ChildrenVillegas Sepúlveda AbrahamNessuna valutazione finora
- Goodpasture Syndrome: Lung and Kidney Autoimmune DiseaseDocumento6 pagineGoodpasture Syndrome: Lung and Kidney Autoimmune DiseaseAman singhNessuna valutazione finora
- AkiDocumento42 pagineAkimarauder_popNessuna valutazione finora
- Blood Conservation Methods in Anaesthesia and SurgeryDocumento113 pagineBlood Conservation Methods in Anaesthesia and SurgeryAgya PrempehNessuna valutazione finora
- What Is LeukemiaDocumento11 pagineWhat Is LeukemiaNazneen RagasaNessuna valutazione finora
- Febrile Neutropenia: Nontapak ThiangpakDocumento53 pagineFebrile Neutropenia: Nontapak ThiangpakRapid MedicineNessuna valutazione finora
- 17 ManuscriptDocumento10 pagine17 ManuscriptBaru Chandrasekhar RaoNessuna valutazione finora
- Pathophysiology 2Documento92 paginePathophysiology 2Princess AgarwalNessuna valutazione finora
- Kwashiorkor AND Marasmus: Group 6Documento18 pagineKwashiorkor AND Marasmus: Group 6Christian De GuzmanNessuna valutazione finora
- Types of Leukemia ExplainedDocumento4 pagineTypes of Leukemia ExplainedwizardebmNessuna valutazione finora
- Acute Myeloid Leukemia (Drug Study)Documento3 pagineAcute Myeloid Leukemia (Drug Study)Krisianne Mae Lorenzo FranciscoNessuna valutazione finora
- Plasminogen ActivatorDocumento3 paginePlasminogen ActivatorteocriNessuna valutazione finora
- Acute Lymphoblastic Leukemia (ALL)Documento14 pagineAcute Lymphoblastic Leukemia (ALL)Med PhuongNessuna valutazione finora
- Leukaemia and Lymphoma Whats The DifferenceDocumento7 pagineLeukaemia and Lymphoma Whats The Differencepaul_calburean7899Nessuna valutazione finora
- Acute Myeloid LekumiaDocumento34 pagineAcute Myeloid LekumiaBhuwan ThapaNessuna valutazione finora
- Nur 111 Session 6 Sas 1Documento12 pagineNur 111 Session 6 Sas 1Zzimply Tri Sha UmaliNessuna valutazione finora
- 13-Cis-Retinoic Acid: It's Therapeutic Implications and Adverse EffectsDocumento8 pagine13-Cis-Retinoic Acid: It's Therapeutic Implications and Adverse EffectsBoston Science Publishing100% (1)
- Systemic Lupus Erythematosus 2012Documento564 pagineSystemic Lupus Erythematosus 2012Dan MunteanuNessuna valutazione finora
- Presentasi CKDDocumento21 paginePresentasi CKDNubli LohNessuna valutazione finora
- Leukemia PDFDocumento63 pagineLeukemia PDFErfan Syahid AzhariNessuna valutazione finora
- Immunopharmacology: Dr. Hamad AlshabiDocumento8 pagineImmunopharmacology: Dr. Hamad AlshabiHamad Alshabi100% (1)
- Haematology - Blood Films.Documento6 pagineHaematology - Blood Films.kkkssbbNessuna valutazione finora
- Normal Lab ValuesDocumento1 paginaNormal Lab Valueshurt_y100% (1)
- Adrenal DisordersDocumento29 pagineAdrenal DisordersSuliman Garalleh100% (1)
- Conventional Versus Video Laryngoscopy For.24Documento9 pagineConventional Versus Video Laryngoscopy For.24Isabella HosanaNessuna valutazione finora
- Nej Mo A 1607991Documento11 pagineNej Mo A 1607991Isabella HosanaNessuna valutazione finora
- ReferencesDocumento1 paginaReferencesIsabella HosanaNessuna valutazione finora
- InformedConsent ClinicalstudiesDocumento10 pagineInformedConsent ClinicalstudiestisconNessuna valutazione finora
- Transcatheter Aortic Valve Replacement With EarlyDocumento2 pagineTranscatheter Aortic Valve Replacement With EarlyIsabella HosanaNessuna valutazione finora
- Pi 3 GammaDocumento11 paginePi 3 GammaIsabella HosanaNessuna valutazione finora
- Anticipated Difficult Airway The Role Of.75Documento2 pagineAnticipated Difficult Airway The Role Of.75Isabella HosanaNessuna valutazione finora
- Laureola LornaDocumento3 pagineLaureola LornaIsabella HosanaNessuna valutazione finora
- Christmas Sponsorship2Documento2 pagineChristmas Sponsorship2Isabella HosanaNessuna valutazione finora
- Mechanisms of Disease in Devt of RaDocumento9 pagineMechanisms of Disease in Devt of RaIsabella HosanaNessuna valutazione finora
- Problem of Choice Current Biologic Agents and Future Prospects in RaDocumento10 pagineProblem of Choice Current Biologic Agents and Future Prospects in RaIsabella HosanaNessuna valutazione finora
- WNT SignalDocumento4 pagineWNT SignalIsabella HosanaNessuna valutazione finora
- Pi 3 GammaDocumento11 paginePi 3 GammaIsabella HosanaNessuna valutazione finora
- Mechanisms of Disease in Devt of RaDocumento9 pagineMechanisms of Disease in Devt of RaIsabella HosanaNessuna valutazione finora
- Cns InfectionsDocumento7 pagineCns InfectionsIsabella HosanaNessuna valutazione finora
- Targetng Intracellular Signaling PathwaysDocumento3 pagineTargetng Intracellular Signaling PathwaysIsabella HosanaNessuna valutazione finora
- Autoimmunity Reviews: ReviewDocumento18 pagineAutoimmunity Reviews: ReviewIsabella HosanaNessuna valutazione finora
- Problem of Choice Current Biologic Agents and Future Prospects in RaDocumento10 pagineProblem of Choice Current Biologic Agents and Future Prospects in RaIsabella HosanaNessuna valutazione finora
- Emerging Cell and Cytokine TargetsDocumento12 pagineEmerging Cell and Cytokine TargetsIsabella HosanaNessuna valutazione finora
- Pathogenesis of Ra From NatureDocumento9 paginePathogenesis of Ra From NatureIsabella HosanaNessuna valutazione finora
- Cns InfectionsDocumento7 pagineCns InfectionsIsabella HosanaNessuna valutazione finora
- Septic Shock - Ongoing Management After Resuscitation in Children - UpToDateDocumento23 pagineSeptic Shock - Ongoing Management After Resuscitation in Children - UpToDateIsabella HosanaNessuna valutazione finora
- Risk of Infection in Children With Fever and Non-chemotherapy-Induced Neutropenia - UpToDateDocumento10 pagineRisk of Infection in Children With Fever and Non-chemotherapy-Induced Neutropenia - UpToDateIsabella HosanaNessuna valutazione finora
- Physiology and Classification of Shock in Children - UpToDateDocumento10 paginePhysiology and Classification of Shock in Children - UpToDateIsabella HosanaNessuna valutazione finora
- Jurnal Tirosin Kinase 4Documento13 pagineJurnal Tirosin Kinase 4Maya SariNessuna valutazione finora
- Chronic Myeloid LeukemiaDocumento12 pagineChronic Myeloid Leukemiaapi-408858450Nessuna valutazione finora
- Haematological Malignancies: Classification, Clinical Features and ManagementDocumento54 pagineHaematological Malignancies: Classification, Clinical Features and ManagementSaifSeddikiNessuna valutazione finora
- How I Treat Mixed-Phenotype Acute LeukemiaDocumento9 pagineHow I Treat Mixed-Phenotype Acute LeukemiaFachitah AndrianicNessuna valutazione finora
- What Was The Human Genome Project?Documento12 pagineWhat Was The Human Genome Project?tonxasNessuna valutazione finora
- Xpert BCR-ABL Ultra: Delivering Confidence With Fast and Accurate Chronic Myeloid Leukemia Molecular Monitoring ResultsDocumento4 pagineXpert BCR-ABL Ultra: Delivering Confidence With Fast and Accurate Chronic Myeloid Leukemia Molecular Monitoring ResultsAndrianRakhmatsyahNessuna valutazione finora
- Medicine 8 - AnswersDocumento111 pagineMedicine 8 - Answersgazelle-xNessuna valutazione finora
- ChemotherapyDocumento16 pagineChemotherapyNandhini SaranathanNessuna valutazione finora
- ДокументDocumento72 pagineДокументDianna ArzumanovaNessuna valutazione finora
- Aj. Chulaporn-Bosutinib-Search Engine and Study EndpointsDocumento5 pagineAj. Chulaporn-Bosutinib-Search Engine and Study EndpointsCalm Phurit SenachaiNessuna valutazione finora
- Digital PCR Application - Leukemia enDocumento10 pagineDigital PCR Application - Leukemia enMohammed H. KeshtaNessuna valutazione finora
- Vox Sanguin Juli 2021Documento124 pagineVox Sanguin Juli 2021rsdarsono labNessuna valutazione finora
- Seminar: Florent Malard, Mohamad MohtyDocumento17 pagineSeminar: Florent Malard, Mohamad MohtyStephania SandovalNessuna valutazione finora
- BCR-ABL Medula OsseaDocumento4 pagineBCR-ABL Medula Osseanathaliasantosx3Nessuna valutazione finora
- 10.1038@s41588 018 0315 5Documento20 pagine10.1038@s41588 018 0315 5Omar FernándezNessuna valutazione finora
- Biology Project CancerDocumento20 pagineBiology Project CancerJay PrakashNessuna valutazione finora
- Directory of Service (DOS) - Effective From 1st April 2012Documento74 pagineDirectory of Service (DOS) - Effective From 1st April 2012kgnmatinNessuna valutazione finora
- Acute Lymphoblastic Leukemia in The Older Adult: Ibrahim Aldoss, MD Stephen J. Forman, MD and Vinod Pullarkat, MDDocumento10 pagineAcute Lymphoblastic Leukemia in The Older Adult: Ibrahim Aldoss, MD Stephen J. Forman, MD and Vinod Pullarkat, MDHugo HectorNessuna valutazione finora
- Understanding Acute Leukemia: Signs, Symptoms and TreatmentDocumento46 pagineUnderstanding Acute Leukemia: Signs, Symptoms and TreatmentMaica LectanaNessuna valutazione finora
- Mechanisms of Resistance To Imatinib and Second-GenerationDocumento10 pagineMechanisms of Resistance To Imatinib and Second-GenerationRiyadh Z. MawloodNessuna valutazione finora
- Chronic Myelogenous Leukemia: The PH ChromosomeDocumento1 paginaChronic Myelogenous Leukemia: The PH ChromosomeJolaine ValloNessuna valutazione finora
- 3讲义hematologyDocumento96 pagine3讲义hematologychongyu888xiongNessuna valutazione finora
- Chronic Myeloid LeukemiaDocumento15 pagineChronic Myeloid Leukemiabonitaeffendi100% (1)