Potrebbero piacerti anche
- ACALASIADocumento34 pagineACALASIAGustavo Bustamante TueroNessuna valutazione finora
- Caso Clínico - Isquemia MesentéricaDocumento36 pagineCaso Clínico - Isquemia MesentéricayemorenoNessuna valutazione finora
- Manual de cirugía bariátrica para profesionales de atención primariaDa EverandManual de cirugía bariátrica para profesionales de atención primariaNessuna valutazione finora
- Cirugia de PancreasDocumento15 pagineCirugia de PancreasLaura MamaniNessuna valutazione finora
- CUCIDocumento50 pagineCUCIManuel GonzalezNessuna valutazione finora
- Colangitis AgudaDocumento5 pagineColangitis AgudaAnthony OsorioNessuna valutazione finora
- Cirugia Examen 20 Preguntas EunacomDocumento14 pagineCirugia Examen 20 Preguntas Eunacomdaveyba89yamparaNessuna valutazione finora
- Malformaciones Ano-RectalesDocumento3 pagineMalformaciones Ano-RectalesJosue Eduardo Bernal MejiaNessuna valutazione finora
- Hemorragia Gastrointestinal GPCDocumento4 pagineHemorragia Gastrointestinal GPCm2rv110Nessuna valutazione finora
- Fisura AnalDocumento13 pagineFisura AnalJocelyn Mercado100% (1)
- Cirugia 6Documento129 pagineCirugia 6Julio César Alvarado FloresNessuna valutazione finora
- Clase Cierre Primario de Vía BiliarDocumento11 pagineClase Cierre Primario de Vía BiliarMaximiliano de OroNessuna valutazione finora
- Derrame Pleural MIRDocumento27 pagineDerrame Pleural MIRRobert100% (1)
- Expo Abdomen AgudoDocumento35 pagineExpo Abdomen AgudoJose Luis Raymundo Perea100% (1)
- Vesicula BiliarDocumento6 pagineVesicula BiliarAntonioNessuna valutazione finora
- Cistograma MiccionalDocumento69 pagineCistograma Miccionaltere serrano0% (1)
- Cancer de Recto 2018Documento88 pagineCancer de Recto 2018Daniel La Concha Rodriguez0% (1)
- Colangitis MonografíaDocumento35 pagineColangitis MonografíaLuis Felipe Huertas100% (1)
- Patología MamariaDocumento49 paginePatología Mamariachrispro24Nessuna valutazione finora
- Ampuloma de WipleDocumento5 pagineAmpuloma de WiplemaidaNessuna valutazione finora
- Evaluación Clínica de Las Masas AnexialesDocumento67 pagineEvaluación Clínica de Las Masas AnexialesJosefa Micaela Gómez De GraciaNessuna valutazione finora
- Patología MamariaDocumento8 paginePatología MamariaPablo Ignacio TamayoNessuna valutazione finora
- PATOLOGÍA ANORRECTAL Clase QXDocumento8 paginePATOLOGÍA ANORRECTAL Clase QXLorena Angarita RamirezNessuna valutazione finora
- Perforacion GastrointestinalDocumento3 paginePerforacion GastrointestinalKevin Verde AredoNessuna valutazione finora
- Casos Clínicos de Gastroenterología PrácticaDocumento6 pagineCasos Clínicos de Gastroenterología PrácticaJulio Cesar Condori TolabaNessuna valutazione finora
- GPC11 DiabetesDocumento14 pagineGPC11 DiabetesGilberto Juvencio Solano Aparicio100% (2)
- RetroperitoneoDocumento61 pagineRetroperitoneoCristianJairValenciaNessuna valutazione finora
- Caso Clinico GastroDocumento12 pagineCaso Clinico GastroDannielGGNessuna valutazione finora
- Cancer de Recto Anatomia QuirurgicaDocumento9 pagineCancer de Recto Anatomia QuirurgicaDannyCespedesNessuna valutazione finora
- Unidades de ElectrocirugíaDocumento43 pagineUnidades de ElectrocirugíaEladioNessuna valutazione finora
- Cancer de PancreasDocumento23 pagineCancer de PancreaslizinkatruyenqueNessuna valutazione finora
- Doppler RenalDocumento17 pagineDoppler RenalSalvador BarahonaNessuna valutazione finora
- Pielografia AscendenteDocumento15 paginePielografia AscendentePaùl Rivera CruzNessuna valutazione finora
- Exploracion de Vias BiliaresDocumento8 pagineExploracion de Vias BiliaresEver Andres Zegarra CandiottiNessuna valutazione finora
- Tesis Fernando 2019 Borrador2Documento36 pagineTesis Fernando 2019 Borrador2MarinaCorderoNessuna valutazione finora
- QuisterDocumento17 pagineQuisterClaudio Castillo CamposNessuna valutazione finora
- Patologia Mamaria BenignaDocumento84 paginePatologia Mamaria BenignaAlicia PizarroNessuna valutazione finora
- CA Pancreas y Cabeza de PancreasDocumento6 pagineCA Pancreas y Cabeza de Pancreaskarla saenzNessuna valutazione finora
- Patologia Del Riñon y Vias Urinarias en EcografiaDocumento49 paginePatologia Del Riñon y Vias Urinarias en EcografiaDavid Mayo Figueroa100% (1)
- Apendicitis ComplicadaDocumento5 pagineApendicitis ComplicadaLuis Puicon Morazzani100% (1)
- Criterios de Transplante PDFDocumento12 pagineCriterios de Transplante PDFAdriana Roa BallesterosNessuna valutazione finora
- Resumen Cirugia GeneralDocumento10 pagineResumen Cirugia GeneralGR StalynNessuna valutazione finora
- Urograma ExcretorDocumento37 pagineUrograma ExcretorcarlosNessuna valutazione finora
- Manejo Del Carro RojoDocumento87 pagineManejo Del Carro RojoMarcela Penques75% (4)
- Ecografia Abdominal A Pie de CamaDocumento8 pagineEcografia Abdominal A Pie de CamaJorge CorreaNessuna valutazione finora
- Cancer de MamaDocumento41 pagineCancer de MamaIman Javier Matos PeñaNessuna valutazione finora
- Bezoares, APUDomas, Trauma GastricoDocumento57 pagineBezoares, APUDomas, Trauma GastricoAlejandro VargasNessuna valutazione finora
- Cancer de Colon y RectoDocumento21 pagineCancer de Colon y RectoHeidi Ferrer VargasNessuna valutazione finora
- Poliposis Intestinal y Cancer de ColonDocumento7 paginePoliposis Intestinal y Cancer de ColonlaurajaimeNessuna valutazione finora
- Hemodinamia Grupo 5Documento15 pagineHemodinamia Grupo 5api-560327902Nessuna valutazione finora
- Cáncer de HígadoDocumento8 pagineCáncer de HígadoStephanie BenitesNessuna valutazione finora
- Fistulas AnalesDocumento28 pagineFistulas AnalesJisse GualánNessuna valutazione finora
- Fiebre PostoperatoriaDocumento15 pagineFiebre PostoperatoriaJose Luis Marin CatacoraNessuna valutazione finora
- Colelitiasis PDFDocumento10 pagineColelitiasis PDFAlecita HummelsNessuna valutazione finora
- Manejo Preoperatorio y TransoperatorioDocumento29 pagineManejo Preoperatorio y TransoperatorioNilia AguilarNessuna valutazione finora
- Vesícula BiliarDocumento16 pagineVesícula BiliarGlen FigueroaNessuna valutazione finora
- Trauma AbdominalDocumento12 pagineTrauma AbdominalSimonGonzalezAponteNessuna valutazione finora
- Dialisis Peritoneal BasesDocumento50 pagineDialisis Peritoneal BasesLaura LizardoNessuna valutazione finora
- Las 7 Formas de Comunicación de La FasciaDocumento1 paginaLas 7 Formas de Comunicación de La FasciaBravo EbsNessuna valutazione finora
- 10 Razones Porqué Rastreos Completos en Lugar Preguntar Pares EspecíficosDocumento1 pagina10 Razones Porqué Rastreos Completos en Lugar Preguntar Pares EspecíficosBravo EbsNessuna valutazione finora
- Ejercicios de PNL para Activar La AlegríaDocumento3 pagineEjercicios de PNL para Activar La AlegríaBravo EbsNessuna valutazione finora
- El Kosmos Según Ken WilberDocumento9 pagineEl Kosmos Según Ken WilberBravo Ebs100% (2)
- Cómo Superar El Miedo Al Abandono Con PNLDocumento3 pagineCómo Superar El Miedo Al Abandono Con PNLBravo EbsNessuna valutazione finora
- ABC en Manejo Del DolorDocumento4 pagineABC en Manejo Del DolorBravo EbsNessuna valutazione finora
- 10 Consejos para Curar Una Casa Enferma y Mantener Un Hogar Sano Y Libre de Energías NegativasDocumento5 pagine10 Consejos para Curar Una Casa Enferma y Mantener Un Hogar Sano Y Libre de Energías NegativasBravo EbsNessuna valutazione finora
- Beneficios Del BerroDocumento6 pagineBeneficios Del BerroBravo EbsNessuna valutazione finora
- Dolor Zona Alta de Columna VertebralDocumento2 pagineDolor Zona Alta de Columna VertebralBravo EbsNessuna valutazione finora
- 12 Errores Más Graves Que Cometen Los Padres Al Educar A Sus HijosDocumento12 pagine12 Errores Más Graves Que Cometen Los Padres Al Educar A Sus HijosBravo Ebs100% (1)
- 8 Estilos CognitivosDocumento4 pagine8 Estilos CognitivosBravo EbsNessuna valutazione finora
- 20 Razones para Tomar Colágeno HidrolizadoDocumento2 pagine20 Razones para Tomar Colágeno HidrolizadoBravo EbsNessuna valutazione finora
- Los Mudras y Sus BeneficiosDocumento26 pagineLos Mudras y Sus BeneficiosBravo EbsNessuna valutazione finora
- Qué Es La Precordialgia No Cardíaca y Cómo Se TrataDocumento21 pagineQué Es La Precordialgia No Cardíaca y Cómo Se TrataBravo EbsNessuna valutazione finora
- Semiología Pediátrica GastrointestinalDocumento20 pagineSemiología Pediátrica GastrointestinalSally Paredes NoguniNessuna valutazione finora
- Acido FusídicoDocumento2 pagineAcido FusídicoFiorella NicolettiNessuna valutazione finora
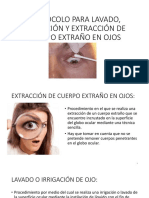
- Lavado Ocular e IrrigaciónDocumento17 pagineLavado Ocular e IrrigaciónJose Eduardo Mejorado ReynaNessuna valutazione finora
- Cientific Hyaluronic Facial Implant 30y18Documento18 pagineCientific Hyaluronic Facial Implant 30y18fatacioliNessuna valutazione finora
- Cuestionario Perfil LipidicoDocumento5 pagineCuestionario Perfil LipidicoMuñoz Landivar Irene50% (2)
- Perls, Ellis y RogersDocumento5 paginePerls, Ellis y RogersDan Perez75% (8)
- AtelectasiaDocumento49 pagineAtelectasiaCarlos Gonzales100% (3)
- Mesa Redonda: Mesa Redonda 3. Síndrome Metabólico. Nuevas Perspectivas de Antiguos ConocidosDocumento14 pagineMesa Redonda: Mesa Redonda 3. Síndrome Metabólico. Nuevas Perspectivas de Antiguos ConocidosGeraldineNessuna valutazione finora
- Síndrome TóxicoDocumento2 pagineSíndrome TóxicoAlejandro GalloNessuna valutazione finora
- Preparación de DextrosaDocumento9 paginePreparación de DextrosaDonaire DuranNessuna valutazione finora
- Sesiones de Aprendizaje, Rubricas, Carpeta PedagógicaDocumento20 pagineSesiones de Aprendizaje, Rubricas, Carpeta PedagógicaAlejandro La Cruz ToledoNessuna valutazione finora
- Pharmabrand (EC) Vs MERCKDocumento5 paginePharmabrand (EC) Vs MERCKdaboNessuna valutazione finora
- Casos Upao - Ginecologia (Dr. Rojas)Documento2 pagineCasos Upao - Ginecologia (Dr. Rojas)Manuel Sachun PlasenciaNessuna valutazione finora
- Clase de Tabaquismo BorradorDocumento24 pagineClase de Tabaquismo Borradorapi-26188232Nessuna valutazione finora
- Caso UltimoDocumento8 pagineCaso UltimoDavid Hurtado33% (3)
- Plan Terapeutico-TlpDocumento68 paginePlan Terapeutico-TlpYohana Maguiña EgusquizaNessuna valutazione finora
- Conciencia Sin FronterasDocumento10 pagineConciencia Sin Fronteraswalter albertNessuna valutazione finora
- Nuevo Triptico Salud MentalDocumento2 pagineNuevo Triptico Salud MentalPancracia López82% (22)
- El Alimento Estrella Semilla de AguacateDocumento2 pagineEl Alimento Estrella Semilla de AguacateMilagros MarquezNessuna valutazione finora
- Manejo Del Dolor en Pediatría, Evaluacion, Tto y Prev Del Dolor (Andalucia)Documento113 pagineManejo Del Dolor en Pediatría, Evaluacion, Tto y Prev Del Dolor (Andalucia)Maria BruningNessuna valutazione finora
- ADME Distribucion Metabolismo y ExcrecionDocumento6 pagineADME Distribucion Metabolismo y ExcrecionCristian Andrés VeraNessuna valutazione finora
- 6 TDAH y TNDDocumento40 pagine6 TDAH y TNDSofía HDNessuna valutazione finora
- Triptico SerpientesDocumento2 pagineTriptico SerpientesSBP Site ManagerNessuna valutazione finora
- Técnicas Plásticas Del Arte Moderno y Arte TerapiaDocumento380 pagineTécnicas Plásticas Del Arte Moderno y Arte Terapiasethiee100% (1)
- Jabon de AvenaDocumento6 pagineJabon de AvenaMarco Sanchez OlayaNessuna valutazione finora
- Hipertensión Portal para SeminarioDocumento70 pagineHipertensión Portal para SeminarioCiro Calviño EstradaNessuna valutazione finora
- Teosyal-FolletoPacientes 1 PDFDocumento8 pagineTeosyal-FolletoPacientes 1 PDFMaartin FoxNessuna valutazione finora
- Desarrollo de Una Metodología Analítica para Determinación Simultánea de Vincristina y Doxorrubicina en Preparaciones Farmacéuticas para Oncología Por HPLCDocumento5 pagineDesarrollo de Una Metodología Analítica para Determinación Simultánea de Vincristina y Doxorrubicina en Preparaciones Farmacéuticas para Oncología Por HPLCMarianaSalgadoNessuna valutazione finora
- Serie y Suplemento - Rodulfo R.Documento12 pagineSerie y Suplemento - Rodulfo R.Vale Marchetti50% (2)
- Que Usos Tienen Las Radiaciones IonizantesDocumento19 pagineQue Usos Tienen Las Radiaciones IonizantesJose Luis Mamani TturoNessuna valutazione finora
- Tus Zonas Erroneas: Guía Para Combatir las Causas de la InfelicidadDa EverandTus Zonas Erroneas: Guía Para Combatir las Causas de la InfelicidadValutazione: 4.5 su 5 stelle4.5/5 (1833)
- Los Secretos De La Mente Millonaria: Domina el juego de la riquezaDa EverandLos Secretos De La Mente Millonaria: Domina el juego de la riquezaValutazione: 5 su 5 stelle5/5 (457)
- Resetea tu mente. Descubre de lo que eres capazDa EverandResetea tu mente. Descubre de lo que eres capazValutazione: 5 su 5 stelle5/5 (196)
- El Monje Que Vendio Su Ferrari: Una Fábula EspiritualDa EverandEl Monje Que Vendio Su Ferrari: Una Fábula EspiritualValutazione: 4.5 su 5 stelle4.5/5 (1699)
- Ayurveda: Descubriendo los Secretos de la Curación Hindú a Través de la Dieta del Ayurveda, el Yoga, la Aromaterapia y la MeditaciónDa EverandAyurveda: Descubriendo los Secretos de la Curación Hindú a Través de la Dieta del Ayurveda, el Yoga, la Aromaterapia y la MeditaciónValutazione: 4 su 5 stelle4/5 (7)
- Guías Espirituales: ¡Una guía para conectarte y comunicarte con tus guías espirituales!Da EverandGuías Espirituales: ¡Una guía para conectarte y comunicarte con tus guías espirituales!Valutazione: 4.5 su 5 stelle4.5/5 (14)
- La metamedicina. Cada síntoma es un mensaje: La curación a tu alcanceDa EverandLa metamedicina. Cada síntoma es un mensaje: La curación a tu alcanceValutazione: 5 su 5 stelle5/5 (8)
- ¡Tómate un respiro! Mindfulness: El arte de mantener la calma en medio de la tempestadDa Everand¡Tómate un respiro! Mindfulness: El arte de mantener la calma en medio de la tempestadValutazione: 5 su 5 stelle5/5 (199)
- Sistema nervioso y osteopatía: Nervios periféricos, meninges craneales y espinales, y sistema nervioso vegetativo (Color)Da EverandSistema nervioso y osteopatía: Nervios periféricos, meninges craneales y espinales, y sistema nervioso vegetativo (Color)Valutazione: 5 su 5 stelle5/5 (9)
- En sintonía con tu ciclo femenino: FLO. Aprende a sincronizarte con tu bioquímica para dar rienda suelta a tu creatividad, mejorar tu vida y hacer más con menos estrésDa EverandEn sintonía con tu ciclo femenino: FLO. Aprende a sincronizarte con tu bioquímica para dar rienda suelta a tu creatividad, mejorar tu vida y hacer más con menos estrésValutazione: 4.5 su 5 stelle4.5/5 (11)
- Escribe el guion de la vida que quieres: Manifiesta tus sueños con tan solo lápiz y papelDa EverandEscribe el guion de la vida que quieres: Manifiesta tus sueños con tan solo lápiz y papelValutazione: 5 su 5 stelle5/5 (1)
- Signos y símbolos: Desvelando el significado espiritual de los sellos angélicos, tótems y otros símbolos mágicos, sagrados y religiososDa EverandSignos y símbolos: Desvelando el significado espiritual de los sellos angélicos, tótems y otros símbolos mágicos, sagrados y religiososValutazione: 5 su 5 stelle5/5 (1)
- ¡Basta ya de ser un Tipo Lindo! (No More Mr. Nice Guy): Un Plan Probado para Que Obtengas Lo Que Quieras en La Vida El Sexo y El Amor (A Proven Plan for Getting What You Want in Love, Sex and Life)Da Everand¡Basta ya de ser un Tipo Lindo! (No More Mr. Nice Guy): Un Plan Probado para Que Obtengas Lo Que Quieras en La Vida El Sexo y El Amor (A Proven Plan for Getting What You Want in Love, Sex and Life)Valutazione: 5 su 5 stelle5/5 (47)
- Entrenamiento Científico con pesas: Fitness InteligenteDa EverandEntrenamiento Científico con pesas: Fitness InteligenteValutazione: 5 su 5 stelle5/5 (3)
- Seguridad en el amor: Cómo superar el apego y la ansiedad en tu relaciónDa EverandSeguridad en el amor: Cómo superar el apego y la ansiedad en tu relaciónValutazione: 4.5 su 5 stelle4.5/5 (76)
- Fuerza de voluntad: Cómo practicar y dominar el autocontrolDa EverandFuerza de voluntad: Cómo practicar y dominar el autocontrolValutazione: 4.5 su 5 stelle4.5/5 (91)
- El oráculo de las diosas: El despertar de lo femenino. Guía de autoconocimientoDa EverandEl oráculo de las diosas: El despertar de lo femenino. Guía de autoconocimientoValutazione: 5 su 5 stelle5/5 (1)
- Batidos Verdes Depurativos y Antioxidantes: Aumenta tu Vitalidad con Smoothie Detox Durante 10 Días Para Adelgazar y Bajar de Peso: Aumenta tu vitalidad con smoothie detox durante 10 días para adelgazar y bajar de pesoDa EverandBatidos Verdes Depurativos y Antioxidantes: Aumenta tu Vitalidad con Smoothie Detox Durante 10 Días Para Adelgazar y Bajar de Peso: Aumenta tu vitalidad con smoothie detox durante 10 días para adelgazar y bajar de pesoValutazione: 5 su 5 stelle5/5 (2)
- Mujeres de luz: Guía para descubrir el poder de tu alma y su propósitoDa EverandMujeres de luz: Guía para descubrir el poder de tu alma y su propósitoValutazione: 4.5 su 5 stelle4.5/5 (39)
- El libro completo de numerología: El descubrimiento del yo interiorDa EverandEl libro completo de numerología: El descubrimiento del yo interiorValutazione: 5 su 5 stelle5/5 (7)
- Una mente en calma: Técnicas para manejar los pensamientos intrusivosDa EverandUna mente en calma: Técnicas para manejar los pensamientos intrusivosValutazione: 4.5 su 5 stelle4.5/5 (142)
- Grimorio: Cómo lanzar y elaborar hechizos mágicos, aprender las prácticas wiccanas y desvelar los secretos de la brujería a través de un diario ritualDa EverandGrimorio: Cómo lanzar y elaborar hechizos mágicos, aprender las prácticas wiccanas y desvelar los secretos de la brujería a través de un diario ritualNessuna valutazione finora