Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Eo Organizing BhertDocumento2 pagineEo Organizing BhertPonciano Alvero95% (21)
- Warehouse Startup ChecklistDocumento3 pagineWarehouse Startup Checklistasgbalaji67% (3)
- Security Guard CVDocumento3 pagineSecurity Guard CVNtubeNessuna valutazione finora
- Funding of Physiotherapy in CanadaDocumento7 pagineFunding of Physiotherapy in Canadawasim.imiNessuna valutazione finora
- AMU Engineering Entrance Exam Physics Solved Paper 2010Documento4 pagineAMU Engineering Entrance Exam Physics Solved Paper 2010BhojNessuna valutazione finora
- Feynman x27 S Tips On Physics Reflections AdviceDocumento2 pagineFeynman x27 S Tips On Physics Reflections AdviceBhojNessuna valutazione finora
- 1 PDFDocumento1 pagina1 PDFBhojNessuna valutazione finora
- How Is A CT Scan Done?Documento4 pagineHow Is A CT Scan Done?BhojNessuna valutazione finora
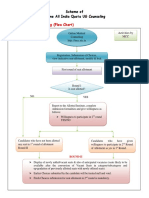
- A. Process of Counseling (Flow Chart) : Scheme of Online All India Quota UG CounselingDocumento21 pagineA. Process of Counseling (Flow Chart) : Scheme of Online All India Quota UG CounselingBhojNessuna valutazione finora
- Unit-III Chapter-10 Cell Structure: Important PointsDocumento13 pagineUnit-III Chapter-10 Cell Structure: Important PointsBhojNessuna valutazione finora
- Connect. Learn. Succeed.: Mcgraw-Hill Higher EducationDocumento3 pagineConnect. Learn. Succeed.: Mcgraw-Hill Higher EducationBhojNessuna valutazione finora
- National Entrance Screening Test: 20, 2008 1.00 PM 4.00 PMDocumento32 pagineNational Entrance Screening Test: 20, 2008 1.00 PM 4.00 PMBhojNessuna valutazione finora
- Entrepreneurship Policy Digest Occupational Licensing: A Barrier To Entrepreneurship (Updated September 2015)Documento2 pagineEntrepreneurship Policy Digest Occupational Licensing: A Barrier To Entrepreneurship (Updated September 2015)The Ewing Marion Kauffman FoundationNessuna valutazione finora
- Domain 2 Financial ManagementDocumento12 pagineDomain 2 Financial ManagementTine CristineNessuna valutazione finora
- 5.5c Infection Control Annual Work Plan 2013-14Documento8 pagine5.5c Infection Control Annual Work Plan 2013-14Tianti PuadiNessuna valutazione finora
- Animal Control Officers and Wild Animals: Incidental CaptureDocumento2 pagineAnimal Control Officers and Wild Animals: Incidental Capturekhers_zalNessuna valutazione finora
- HRM Chapter 5Documento14 pagineHRM Chapter 5Bibi Jamiatun MohamadNessuna valutazione finora
- Pages440-442 bshb09 EaglerrsDocumento3 paginePages440-442 bshb09 Eaglerrsapi-254133492Nessuna valutazione finora
- DR RadhakrishnaDocumento74 pagineDR RadhakrishnaChandra ReddyNessuna valutazione finora
- About GSK inDocumento6 pagineAbout GSK inFaisal ParachaNessuna valutazione finora
- All India Hospital ListDocumento554 pagineAll India Hospital ListdrsdubeyNessuna valutazione finora
- EN14901 Epoxy Externally Coated Ductile Iron PipesDocumento24 pagineEN14901 Epoxy Externally Coated Ductile Iron Pipesuputsvo52Nessuna valutazione finora
- Go Ms No14Documento5 pagineGo Ms No14rajuNessuna valutazione finora
- Notes On Reading STCW95: - Français Deutsch Nederlands Español ItalianoDocumento6 pagineNotes On Reading STCW95: - Français Deutsch Nederlands Español ItalianoHan Thu WynnNessuna valutazione finora
- FAO - Environmental Impact Assessment and Monitoring in Aquaculture - TP 527Documento675 pagineFAO - Environmental Impact Assessment and Monitoring in Aquaculture - TP 527g4nz0100% (2)
- Glossary: Agency - Certified Home Health Care Agencies. Certified Home Health AgenciesDocumento8 pagineGlossary: Agency - Certified Home Health Care Agencies. Certified Home Health AgenciesLinda RodriguezNessuna valutazione finora
- Tanggung Jawab Apoteker Pengelolaapotek Terhadap Tindakan Wanprestasi Dalam Perjanjian Kerjasama Dengan Pemilik Sarana Apotek "Musuk Farma" BoyolaliDocumento9 pagineTanggung Jawab Apoteker Pengelolaapotek Terhadap Tindakan Wanprestasi Dalam Perjanjian Kerjasama Dengan Pemilik Sarana Apotek "Musuk Farma" BoyolaliMaulinaNessuna valutazione finora
- Proposed Rule: Legal Assistance Eligibility Maximum Income GuidelinesDocumento16 pagineProposed Rule: Legal Assistance Eligibility Maximum Income GuidelinesJustia.com100% (1)
- CHAPTER 7 Unit 2 Income and Careers Chapter 7 Insuring Your Health and Your Life-LessonDocumento12 pagineCHAPTER 7 Unit 2 Income and Careers Chapter 7 Insuring Your Health and Your Life-LessonAnn RosoladaNessuna valutazione finora
- Global Population (Revised)Documento25 pagineGlobal Population (Revised)Salman PreeomNessuna valutazione finora
- Feminist UBI - CNDI 2023Documento76 pagineFeminist UBI - CNDI 2023aimans.indigoNessuna valutazione finora
- Appointment DocumentDocumento5 pagineAppointment Documentaamir khan100% (2)
- 2Documento43 pagine2guluNessuna valutazione finora
- Project Design PNP FoodDocumento3 pagineProject Design PNP FoodAllen Lucre ReondangaNessuna valutazione finora
- Course Outline - 2015 - Medical and Health LawDocumento10 pagineCourse Outline - 2015 - Medical and Health LawAnonymous krdEqdNessuna valutazione finora
- Ashridge Corporate BrochureDocumento25 pagineAshridge Corporate BrochureakankshaiNessuna valutazione finora
- 115-Orate vs. CA, Et - Al.Documento7 pagine115-Orate vs. CA, Et - Al.Nimpa PichayNessuna valutazione finora
- Tele MedicineDocumento12 pagineTele MedicineNoorul Faedzah RosliNessuna valutazione finora