Potrebbero piacerti anche
- Content ServerDocumento5 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
- Comparison of Dentinal Damage Induced by Different Nickel-Titanium Rotary Instruments During Canal Preparation: An in Vitro StudyDocumento4 pagineComparison of Dentinal Damage Induced by Different Nickel-Titanium Rotary Instruments During Canal Preparation: An in Vitro StudyAmee PatelNessuna valutazione finora
- Micro-Computed Tomographic Analysis of Apical Foramen Enlargement of Mature Teeth: A Cadaveric StudyDocumento6 pagineMicro-Computed Tomographic Analysis of Apical Foramen Enlargement of Mature Teeth: A Cadaveric StudyJonatan VelezNessuna valutazione finora
- 27 Sadashiv DaokarDocumento7 pagine27 Sadashiv DaokarMihaela TuculinaNessuna valutazione finora
- Jurnal Apical GaugingDocumento9 pagineJurnal Apical GaugingRara SarahNessuna valutazione finora
- CLR 33 353Documento9 pagineCLR 33 353Paul PalomequeNessuna valutazione finora
- Articulos Traducidos AnnyyyDocumento32 pagineArticulos Traducidos AnnyyyNahomi ConsueloNessuna valutazione finora
- Alignment Efficiency and Esthetic Performance of 4 2017 American Journal ofDocumento9 pagineAlignment Efficiency and Esthetic Performance of 4 2017 American Journal ofdruzair007Nessuna valutazione finora
- The Effect of Root Canal Preparation On The Development of Dentin CracksDocumento6 pagineThe Effect of Root Canal Preparation On The Development of Dentin CracksRespiika YuliaaNessuna valutazione finora
- Time To Rethink: Dr. Suchita S. Daokar, Dr. Handa Amit Satish, Dr. Sunita SachdeoDocumento6 pagineTime To Rethink: Dr. Suchita S. Daokar, Dr. Handa Amit Satish, Dr. Sunita SachdeoShinta PurnamasariNessuna valutazione finora
- Efficiency of Upper Arch Expansion With The Invisalign SystemDocumento8 pagineEfficiency of Upper Arch Expansion With The Invisalign SystemReinaldo Morocho MontalvánNessuna valutazione finora
- InstrumentationDocumento12 pagineInstrumentationMaiush JbNessuna valutazione finora
- Stereomicroscopic Evaluation of Dentinal Defects Induced by New Rotary System: "Protaper Next"Documento4 pagineStereomicroscopic Evaluation of Dentinal Defects Induced by New Rotary System: "Protaper Next"Amee PatelNessuna valutazione finora
- Boeddinghaus 2015Documento8 pagineBoeddinghaus 2015wellington_cmlNessuna valutazione finora
- Laser Tooth Preparation For Pit and Fissure Sealing: Environmental Research and Public HealthDocumento11 pagineLaser Tooth Preparation For Pit and Fissure Sealing: Environmental Research and Public HealthFikrisalsabilahmahmudNessuna valutazione finora
- A Study of Root Canal Morphology of Human Primary Molars Using Computerised Tomography - An in Vitro Study Zoremchhingi, Joseph T, Varma B, Mungara J - J Indian Soc Pedod Prev DentDocumento8 pagineA Study of Root Canal Morphology of Human Primary Molars Using Computerised Tomography - An in Vitro Study Zoremchhingi, Joseph T, Varma B, Mungara J - J Indian Soc Pedod Prev DentyeeruiNessuna valutazione finora
- Alignment Efficiency and Discomfort of Three Orthodontic Archwire Sequences: A Randomized Clinical TrialDocumento8 pagineAlignment Efficiency and Discomfort of Three Orthodontic Archwire Sequences: A Randomized Clinical TrialFaraz SayedNessuna valutazione finora
- The Role of Apical Instrumentation in Root Canal Treatment - A Review of The Literature-286-270Documento8 pagineThe Role of Apical Instrumentation in Root Canal Treatment - A Review of The Literature-286-270rojek63Nessuna valutazione finora
- NEW BUSHRA FinalDocumento22 pagineNEW BUSHRA Finalmudassir rehman100% (1)
- Evaluation of Fracture Resistance of Mandibular Premolar Canals Filled With Four Different Obturation Techniques-An in Vitro StudyDocumento6 pagineEvaluation of Fracture Resistance of Mandibular Premolar Canals Filled With Four Different Obturation Techniques-An in Vitro StudyNatalia MosqueraNessuna valutazione finora
- Prevalence of Elongation and Calcification Patterns of Elongated Styloid Process in South IndiaDocumento6 paginePrevalence of Elongation and Calcification Patterns of Elongated Styloid Process in South IndiaEl GalenoNessuna valutazione finora
- Jurnal Prepasi Saluran AkarDocumento7 pagineJurnal Prepasi Saluran AkarRespiika YuliaaNessuna valutazione finora
- Twisted Vs Protaper Files in Contemporary Pediatric EndodonticsDocumento4 pagineTwisted Vs Protaper Files in Contemporary Pediatric EndodonticsrizkazaimNessuna valutazione finora
- Extraoral Radiography An Alternative To Intraoral Radiography For Endodontic (Root Canal System) Length DeterminationDocumento11 pagineExtraoral Radiography An Alternative To Intraoral Radiography For Endodontic (Root Canal System) Length DeterminationsevattapillaiNessuna valutazione finora
- Prospective Observational Titanium Dental Implants in An Indian ContextDocumento8 pagineProspective Observational Titanium Dental Implants in An Indian ContextTJPRC PublicationsNessuna valutazione finora
- Study of Endodontic Working Length of Korean Posterior TeethDocumento7 pagineStudy of Endodontic Working Length of Korean Posterior TeethPavan TenglikarNessuna valutazione finora
- Instrument Separation Analysis of Multi-Used Protaper Universal Rotary System During Root Canal TherapyDocumento6 pagineInstrument Separation Analysis of Multi-Used Protaper Universal Rotary System During Root Canal TherapyShoaib YounusNessuna valutazione finora
- 1 s2.0 S0917239417301738 MainDocumento7 pagine1 s2.0 S0917239417301738 MainAlison ContrerasNessuna valutazione finora
- 7thpublication IOSR JDMS 1stnameDocumento5 pagine7thpublication IOSR JDMS 1stnameAle GNessuna valutazione finora
- Endodontic ArmamentariumDocumento29 pagineEndodontic ArmamentariumAbdulSamiNessuna valutazione finora
- Journal Club: Dr. Balarama Krishna Academic JR Department of Dentistry AIIMS, BhubaneswarDocumento36 pagineJournal Club: Dr. Balarama Krishna Academic JR Department of Dentistry AIIMS, Bhubaneswarbalarama krishnaNessuna valutazione finora
- 2 Retenedores MandibularesDocumento7 pagine2 Retenedores MandibularesNeiba RomeroNessuna valutazione finora
- + 2016 EJO McNamara - Three-Dimensional Digital Cast Analysis of The Effects Produced by A Passive Self-Ligating SystemDocumento6 pagine+ 2016 EJO McNamara - Three-Dimensional Digital Cast Analysis of The Effects Produced by A Passive Self-Ligating SystemGeorge JoseNessuna valutazione finora
- K File, MtwoDocumento5 pagineK File, MtwoSIDHANT PATHAKNessuna valutazione finora
- Articulo Arco de CantoDocumento7 pagineArticulo Arco de CantoLAURA MARCELA BARRENECHE CALLENessuna valutazione finora
- Maxillary Dentoalveolar Assessment Following Retraction of Maxillary Incisors: A Preliminary StudyDocumento8 pagineMaxillary Dentoalveolar Assessment Following Retraction of Maxillary Incisors: A Preliminary StudyAndrea TokumotoNessuna valutazione finora
- Drakeetal ISNR2012 Dentistry Orthodontic Tooth Movementwith Clear AlignersDocumento8 pagineDrakeetal ISNR2012 Dentistry Orthodontic Tooth Movementwith Clear AlignersLuis SanchezNessuna valutazione finora
- Comparison of The Dental and Skeletal Changes Associated With Maxillary Molar Distalization by Four Different Appliances: An in Vivo StudyDocumento8 pagineComparison of The Dental and Skeletal Changes Associated With Maxillary Molar Distalization by Four Different Appliances: An in Vivo StudyrohitNessuna valutazione finora
- Short-And Long-Term Evaluation of Mandibular Dental Arch Dimensional Changes in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesDocumento8 pagineShort-And Long-Term Evaluation of Mandibular Dental Arch Dimensional Changes in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesGABRIELA NIETO GONZALEZNessuna valutazione finora
- The Influence of The Usage of A Trephine Bar For Dental Implant PlacementDocumento5 pagineThe Influence of The Usage of A Trephine Bar For Dental Implant PlacementKailash VirNessuna valutazione finora
- Dentinal Defects Before and After Rotary Root Canal Instrumentation With Three Different Obturation Techniques and Two Obturating MaterialsDocumento5 pagineDentinal Defects Before and After Rotary Root Canal Instrumentation With Three Different Obturation Techniques and Two Obturating MaterialsAmee PatelNessuna valutazione finora
- A Comparative Study of Vertical Fracture of Roots Obturated With New Obturating Systems - An in Vitro StudyDocumento6 pagineA Comparative Study of Vertical Fracture of Roots Obturated With New Obturating Systems - An in Vitro StudyAmee PatelNessuna valutazione finora
- Mini-Implant Supported Canine Retraction With Micro-Osteoperforation: A Split-Mouth Randomized Clinical TrialDocumento7 pagineMini-Implant Supported Canine Retraction With Micro-Osteoperforation: A Split-Mouth Randomized Clinical Triallaura velez0% (1)
- Effect of ProTaper Universal, Endoflare, Revo-S, HyFlexDocumento3 pagineEffect of ProTaper Universal, Endoflare, Revo-S, HyFlexshamshuddin patelNessuna valutazione finora
- Effect of Different Denture Base - Es.enDocumento6 pagineEffect of Different Denture Base - Es.enCarolina León VásquezNessuna valutazione finora
- 0.018-Inch Vs 0.022-Inch Slot 2Documento11 pagine0.018-Inch Vs 0.022-Inch Slot 2Arkajit GoswamiNessuna valutazione finora
- Dietrich Surgical Extrusion Journal Prosthetic DentistryDocumento38 pagineDietrich Surgical Extrusion Journal Prosthetic DentistryGifix GifunNessuna valutazione finora
- Long-Term Space Changes After Premature Loss of A Primary Maxillary First MolarDocumento5 pagineLong-Term Space Changes After Premature Loss of A Primary Maxillary First MolarFernanda OchoaNessuna valutazione finora
- Clinical Oral Implants Res - 2022 - Lamperti - Cemented Versus Screw Retained Zirconia Based Single Implant RestorationsDocumento9 pagineClinical Oral Implants Res - 2022 - Lamperti - Cemented Versus Screw Retained Zirconia Based Single Implant RestorationsIsaac MoNessuna valutazione finora
- 1 s2.0 S2212443814000186 Main 2Documento6 pagine1 s2.0 S2212443814000186 Main 2Pau ContrerasNessuna valutazione finora
- Arora Et Al. 2012Documento12 pagineArora Et Al. 2012Nawaf RuwailiNessuna valutazione finora
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocumento11 pagineRajiv Gandhi University of Health Sciences Bangalore, Karnatakadrvivek reddyNessuna valutazione finora
- Biomechanical Behavior of TitaniumDocumento7 pagineBiomechanical Behavior of TitaniumDental Del NorteNessuna valutazione finora
- S - 2018 - Accuracy of Newly Developed Sleeve-Designed Templates For Insertion of Dental ImplantsDocumento6 pagineS - 2018 - Accuracy of Newly Developed Sleeve-Designed Templates For Insertion of Dental ImplantsVõHoàngThủyTiênNessuna valutazione finora
- Articulo Sellante InvasivoDocumento7 pagineArticulo Sellante InvasivoJeannette BorreroNessuna valutazione finora
- Effects of Gates-Glidden, LA Axxess and Orifice Shaper Burs On The Cervical Dentin Thickness and Root Canal Area of Mandibular MolarsDocumento4 pagineEffects of Gates-Glidden, LA Axxess and Orifice Shaper Burs On The Cervical Dentin Thickness and Root Canal Area of Mandibular Molarspatel keralNessuna valutazione finora
- Clinical and Patient-Related Outcomes of A Tapered Implant System With Switched Platform Conical Abutments: A Private Practice Field TrialDocumento4 pagineClinical and Patient-Related Outcomes of A Tapered Implant System With Switched Platform Conical Abutments: A Private Practice Field TrialBagis Emre GulNessuna valutazione finora
- Determining The Optimal Length of The Tooth's Root Canal ObturationDocumento7 pagineDetermining The Optimal Length of The Tooth's Root Canal ObturationBogdanNessuna valutazione finora
- Fisher 10 Años RCT HibridaDocumento11 pagineFisher 10 Años RCT HibridaCarlos NaupariNessuna valutazione finora
- Fixed Orthodontic Appliances: A Practical GuideDa EverandFixed Orthodontic Appliances: A Practical GuideValutazione: 1 su 5 stelle1/5 (1)
- Diff Betwn Inlay and Amalgam CavityDocumento7 pagineDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Criteria of SelectionDocumento12 pagineCriteria of SelectionVinisha Vipin SharmaNessuna valutazione finora
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocumento6 pagineNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNessuna valutazione finora
- Challenges in Working Length DeterminationDocumento101 pagineChallenges in Working Length DeterminationVinisha Vipin SharmaNessuna valutazione finora
- Acupuncture in Dentistry PDFDocumento73 pagineAcupuncture in Dentistry PDFVinisha Vipin SharmaNessuna valutazione finora
- Eaat 14 I 1 P 217Documento6 pagineEaat 14 I 1 P 217Vinisha Vipin SharmaNessuna valutazione finora
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocumento159 pagineMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaNessuna valutazione finora
- Glide Path PreparationDocumento5 pagineGlide Path PreparationVinisha Vipin SharmaNessuna valutazione finora
- Some Basics of LasersDocumento102 pagineSome Basics of LasersVinisha Vipin SharmaNessuna valutazione finora
- Show TextDocumento1 paginaShow TextVinisha Vipin SharmaNessuna valutazione finora
- Laser in Conservative Dentistry & EndodonticsDocumento75 pagineLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaNessuna valutazione finora
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocumento5 pagineNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaNessuna valutazione finora
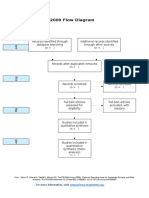
- PRISMA 2009 Flow Diagram: For More Information, VisitDocumento1 paginaPRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaNessuna valutazione finora
- Dentin HypersensitivityDocumento62 pagineDentin HypersensitivityVinisha Vipin Sharma100% (1)
- EchsDocumento20 pagineEchsVinisha Vipin SharmaNessuna valutazione finora
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocumento5 pagineCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaNessuna valutazione finora
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDocumento5 paginePractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaNessuna valutazione finora
- PRISMA-P Statement - Moher Sys Rev Jan 2015Documento9 paginePRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaNessuna valutazione finora
- Pin Retained RestorationDocumento31 paginePin Retained RestorationVinisha Vipin SharmaNessuna valutazione finora
- Esthetic Alternatives To AmalgamDocumento15 pagineEsthetic Alternatives To AmalgamVinisha Vipin SharmaNessuna valutazione finora
- Clarks Cavity PreparationDocumento10 pagineClarks Cavity PreparationVinisha Vipin SharmaNessuna valutazione finora