Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Diff Betwn Inlay and Amalgam CavityDocumento7 pagineDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Acupuncture in Dentistry PDFDocumento73 pagineAcupuncture in Dentistry PDFVinisha Vipin SharmaNessuna valutazione finora
- Criteria of SelectionDocumento12 pagineCriteria of SelectionVinisha Vipin SharmaNessuna valutazione finora
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocumento6 pagineNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNessuna valutazione finora
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocumento159 pagineMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaNessuna valutazione finora
- Eaat 14 I 1 P 217Documento6 pagineEaat 14 I 1 P 217Vinisha Vipin SharmaNessuna valutazione finora
- Some Basics of LasersDocumento102 pagineSome Basics of LasersVinisha Vipin SharmaNessuna valutazione finora
- EchsDocumento20 pagineEchsVinisha Vipin SharmaNessuna valutazione finora
- Challenges in Working Length DeterminationDocumento101 pagineChallenges in Working Length DeterminationVinisha Vipin SharmaNessuna valutazione finora
- Show TextDocumento1 paginaShow TextVinisha Vipin SharmaNessuna valutazione finora
- Glide Path PreparationDocumento5 pagineGlide Path PreparationVinisha Vipin SharmaNessuna valutazione finora
- Content ServerDocumento5 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
- Laser in Conservative Dentistry & EndodonticsDocumento75 pagineLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaNessuna valutazione finora
- Content ServerDocumento6 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
- Dentin HypersensitivityDocumento62 pagineDentin HypersensitivityVinisha Vipin Sharma100% (1)
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDocumento5 paginePractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaNessuna valutazione finora
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocumento5 pagineCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaNessuna valutazione finora
- PRISMA-P Statement - Moher Sys Rev Jan 2015Documento9 paginePRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaNessuna valutazione finora
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocumento5 pagineNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaNessuna valutazione finora
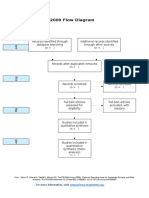
- PRISMA 2009 Flow Diagram: For More Information, VisitDocumento1 paginaPRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaNessuna valutazione finora
- Clarks Cavity PreparationDocumento10 pagineClarks Cavity PreparationVinisha Vipin SharmaNessuna valutazione finora
- Esthetic Alternatives To AmalgamDocumento15 pagineEsthetic Alternatives To AmalgamVinisha Vipin SharmaNessuna valutazione finora
- Pin Retained RestorationDocumento31 paginePin Retained RestorationVinisha Vipin SharmaNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Ergatividad Del Vasco, Teoría Del CasoDocumento58 pagineErgatividad Del Vasco, Teoría Del CasoCristian David Urueña UribeNessuna valutazione finora
- Clearing Negative SpiritsDocumento6 pagineClearing Negative SpiritsmehorseblessedNessuna valutazione finora
- PMS Past Paper Pakistan Studies 2019Documento3 paginePMS Past Paper Pakistan Studies 2019AsmaMaryamNessuna valutazione finora
- Introduction To ICT EthicsDocumento8 pagineIntroduction To ICT EthicsJohn Niño FilipinoNessuna valutazione finora
- Marketing PlanDocumento41 pagineMarketing PlanMark AbainzaNessuna valutazione finora
- Thesis FulltextDocumento281 pagineThesis FulltextEvgenia MakantasiNessuna valutazione finora
- Batch 4 PPTDocumento20 pagineBatch 4 PPTAbhi ShekNessuna valutazione finora
- GearsDocumento14 pagineGearsZulhilmi Chik TakNessuna valutazione finora
- Abnormal PsychologyDocumento13 pagineAbnormal PsychologyBai B. UsmanNessuna valutazione finora
- Your Free Buyer Persona TemplateDocumento8 pagineYour Free Buyer Persona Templateel_nakdjoNessuna valutazione finora
- Process of CounsellingDocumento15 pagineProcess of CounsellingSamuel Njenga100% (1)
- Is 13779 1999 PDFDocumento46 pagineIs 13779 1999 PDFchandranmuthuswamyNessuna valutazione finora
- Chhabra, D., Healy, R., & Sills, E. (2003) - Staged Authenticity and Heritage Tourism. Annals of Tourism Research, 30 (3), 702-719 PDFDocumento18 pagineChhabra, D., Healy, R., & Sills, E. (2003) - Staged Authenticity and Heritage Tourism. Annals of Tourism Research, 30 (3), 702-719 PDF余鸿潇Nessuna valutazione finora
- The Recipe For Oleander Sou1Documento4 pagineThe Recipe For Oleander Sou1Anthony SullivanNessuna valutazione finora
- SHS11Q4DLP 21st CentFinalDocumento33 pagineSHS11Q4DLP 21st CentFinalNOEMI DE CASTRONessuna valutazione finora
- Robot MecanumDocumento4 pagineRobot MecanumalienkanibalNessuna valutazione finora
- Lite Touch. Completo PDFDocumento206 pagineLite Touch. Completo PDFkerlystefaniaNessuna valutazione finora
- WO 2021/158698 Al: (10) International Publication NumberDocumento234 pagineWO 2021/158698 Al: (10) International Publication Numberyoganayagi209Nessuna valutazione finora
- Chinese AstronomyDocumento13 pagineChinese Astronomyss13Nessuna valutazione finora
- Counselling Goes To The Movies: Antwone Fisher (2002)Documento12 pagineCounselling Goes To The Movies: Antwone Fisher (2002)Azizul MohamadNessuna valutazione finora
- Tamil and BrahminsDocumento95 pagineTamil and BrahminsRavi Vararo100% (1)
- Re CrystallizationDocumento25 pagineRe CrystallizationMarol CerdaNessuna valutazione finora
- Origin of "ERP"Documento4 pagineOrigin of "ERP"kanika_bhardwaj_2Nessuna valutazione finora
- Star QuizDocumento3 pagineStar Quizapi-254428474Nessuna valutazione finora
- Design Thinking PDFDocumento7 pagineDesign Thinking PDFFernan SantosoNessuna valutazione finora
- The 5 RS:: A New Teaching Approach To Encourage Slowmations (Student-Generated Animations) of Science ConceptsDocumento7 pagineThe 5 RS:: A New Teaching Approach To Encourage Slowmations (Student-Generated Animations) of Science Conceptsnmsharif66Nessuna valutazione finora
- Influencing Factors Behind The Criminal Attitude: A Study of Central Jail PeshawarDocumento13 pagineInfluencing Factors Behind The Criminal Attitude: A Study of Central Jail PeshawarAmir Hamza KhanNessuna valutazione finora
- Reported Speech StatementsDocumento1 paginaReported Speech StatementsEmilijus Bartasevic100% (1)
- War Thesis StatementsDocumento8 pagineWar Thesis StatementsHelpPaperRochester100% (2)
- Functions & Role of Community Mental Health Nursing: Srinivasan ADocumento29 pagineFunctions & Role of Community Mental Health Nursing: Srinivasan AsrinivasanaNessuna valutazione finora