Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Avian Medicine and Surgery in Practice Companion and Aviary BirdsDocumento384 pagineAvian Medicine and Surgery in Practice Companion and Aviary BirdsDrogaria Econômica0% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Thoughts and AdviceDocumento92 pagineThoughts and AdviceRohit SharmaNessuna valutazione finora
- Differential Diagnosis of Glomerular DiseasesDocumento2 pagineDifferential Diagnosis of Glomerular DiseasesMaryam Fadah100% (1)
- Orthostatic HypotensionDocumento9 pagineOrthostatic HypotensionأحمدالشحاتNessuna valutazione finora
- MRCP Material Drive PDFDocumento2 pagineMRCP Material Drive PDFأحمدالشحات100% (1)
- Chapter 6 - Immune Diseases (Part II) (Robbins and Cotran Pathologic Basis of Disease)Documento3 pagineChapter 6 - Immune Diseases (Part II) (Robbins and Cotran Pathologic Basis of Disease)Ernie G. Bautista II, RN, MD100% (5)
- Amyloidosis: Marwa Bawab - SP 10Documento51 pagineAmyloidosis: Marwa Bawab - SP 10Marrouch Ba100% (1)
- MCQ Bacteriology 31Documento9 pagineMCQ Bacteriology 31أحمدالشحات100% (1)
- Anatomopathological Session: Case 4 - A 79-Year-Old Man With Congestive Heart Failure Due To Restrictive CardiomyopathyDocumento10 pagineAnatomopathological Session: Case 4 - A 79-Year-Old Man With Congestive Heart Failure Due To Restrictive CardiomyopathyNovie AstiniNessuna valutazione finora
- 6 - Immune Deficiency Diseases 2Documento8 pagine6 - Immune Deficiency Diseases 2Belle Galao GepteNessuna valutazione finora
- OphthslDocumento1 paginaOphthslأحمدالشحاتNessuna valutazione finora
- اشهر اسئله لدكتور دينا شكرىDocumento6 pagineاشهر اسئله لدكتور دينا شكرىأحمدالشحاتNessuna valutazione finora
- Set 3c271ab3Documento12 pagineSet 3c271ab3أحمدالشحاتNessuna valutazione finora
- Amiloidosis JAMA 2020Documento11 pagineAmiloidosis JAMA 2020Matías Jesús Flamm ZamoranoNessuna valutazione finora
- MCI FMGE Previous Year Solved Question Paper 2005 MarchDocumento0 pagineMCI FMGE Previous Year Solved Question Paper 2005 MarchSharat Chandra0% (1)
- Aortic Valve Disease, Transcatheter Aortic Valve Replacement, and The Heart Failure Patient A State-Of-The-Art ReviewDocumento14 pagineAortic Valve Disease, Transcatheter Aortic Valve Replacement, and The Heart Failure Patient A State-Of-The-Art ReviewCarlos Alberto Holguin PalaciosNessuna valutazione finora
- Atlas de Marcadores Tumorales - DakoDocumento120 pagineAtlas de Marcadores Tumorales - Dakodavlab76Nessuna valutazione finora
- Internal Medicine Orals E&a Academia (Exclusive)Documento209 pagineInternal Medicine Orals E&a Academia (Exclusive)Shreya SinghNessuna valutazione finora
- MRP 2017Documento175 pagineMRP 2017vk100% (1)
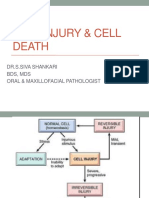
- Cell Injury & Cell DeathDocumento61 pagineCell Injury & Cell DeathshivarocksNessuna valutazione finora
- 2022 AHA/ACC/HFSA Guideline For The Management of Heart Failure: Executive SummaryDocumento24 pagine2022 AHA/ACC/HFSA Guideline For The Management of Heart Failure: Executive SummaryAna RuizNessuna valutazione finora
- 1.inflammation & Repair: Cardinal Signs of InflammationDocumento47 pagine1.inflammation & Repair: Cardinal Signs of Inflammationsharu4291Nessuna valutazione finora
- ASNC AND EANM Amyloidosis Practice Points WEBDocumento12 pagineASNC AND EANM Amyloidosis Practice Points WEBElena FlorentinaNessuna valutazione finora
- EULAR Recommendations For The Management of Familial Mediterranean FeverDocumento8 pagineEULAR Recommendations For The Management of Familial Mediterranean FeverTurboNessuna valutazione finora
- Enfermedad Renal y Desordenes HematologicasDocumento11 pagineEnfermedad Renal y Desordenes HematologicasIris GzlzNessuna valutazione finora
- Quick Review PDFDocumento154 pagineQuick Review PDFDr PenCaster100% (1)
- AMYLOIDOSISDocumento22 pagineAMYLOIDOSISMohan ChoudharyNessuna valutazione finora
- 612 FullDocumento5 pagine612 FullthiagoNessuna valutazione finora
- Biomarkers in AmyloidosisDocumento11 pagineBiomarkers in AmyloidosisMathew McCarthyNessuna valutazione finora
- Journal Reading Clinicopathological Study of Lichen Amyloidosis - Kartika Mega Utami BouwDocumento4 pagineJournal Reading Clinicopathological Study of Lichen Amyloidosis - Kartika Mega Utami BouwmarinNessuna valutazione finora
- Review Articles: Medical ProgressDocumento12 pagineReview Articles: Medical ProgressmoiNessuna valutazione finora
- Path Anat Part 1Documento184 paginePath Anat Part 1Javier Saad100% (1)
- Pathology SWT 13.11. 2023Documento19 paginePathology SWT 13.11. 2023Teena VajiNessuna valutazione finora
- AmyloidosisDocumento5 pagineAmyloidosisVenkata Subramanyam RNessuna valutazione finora
- Morpho KrokDocumento106 pagineMorpho KrokPrashant SinghNessuna valutazione finora