Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- 10 Killer Tips For Transcribing Jazz Solos - Jazz AdviceDocumento21 pagine10 Killer Tips For Transcribing Jazz Solos - Jazz Advicecdmb100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Automatic Gearbox ZF 4HP 20Documento40 pagineAutomatic Gearbox ZF 4HP 20Damien Jorgensen100% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Axera D06Documento2 pagineAxera D06Cristián Fernando Cristóbal RoblesNessuna valutazione finora
- Soil Guidance NotesDocumento18 pagineSoil Guidance Notesసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Account Statement 250820 240920 PDFDocumento2 pagineAccount Statement 250820 240920 PDFUnknown100% (1)
- HRMDocumento118 pagineHRMKarthic KasiliaNessuna valutazione finora
- Pulmonary EmbolismDocumento48 paginePulmonary Embolismganga2424100% (3)
- Babe Ruth Saves BaseballDocumento49 pagineBabe Ruth Saves BaseballYijun PengNessuna valutazione finora
- Union Test Prep Nclex Study GuideDocumento115 pagineUnion Test Prep Nclex Study GuideBradburn Nursing100% (2)
- Rural Poultry Management GuideDocumento7 pagineRural Poultry Management Guideసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Seabank Statement 20220726Documento4 pagineSeabank Statement 20220726Alesa WahabappNessuna valutazione finora
- Roxas City For Revision Research 7 Q1 MELC 23 Week2Documento10 pagineRoxas City For Revision Research 7 Q1 MELC 23 Week2Rachele DolleteNessuna valutazione finora
- Importance of Carrier For Feed Premixes ProductionDocumento5 pagineImportance of Carrier For Feed Premixes Productionసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Avian Respiratory System - EXtensionDocumento3 pagineAvian Respiratory System - EXtensionసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Chicken Anatomy and Physiology: Respiratory System: by Jacquie Jacob and Tony PescatoreDocumento4 pagineChicken Anatomy and Physiology: Respiratory System: by Jacquie Jacob and Tony Pescatoreసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Avian Respiratory System: Jacquie Jacob and Tony Pescatore, Animal SciencesDocumento2 pagineAvian Respiratory System: Jacquie Jacob and Tony Pescatore, Animal Sciencesసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Flavonoid: 1 BiosynthesisDocumento12 pagineFlavonoid: 1 Biosynthesisసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Technote 7 Teat DisinfectionDocumento20 pagineTechnote 7 Teat Disinfectionసాయిమహేష్రెడ్డిఆవుల100% (1)
- Urinary Gamma-Glutamyl Transferase and The Degree of Renal Dysfunction in 75 Bitches With PyometraDocumento32 pagineUrinary Gamma-Glutamyl Transferase and The Degree of Renal Dysfunction in 75 Bitches With Pyometraసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
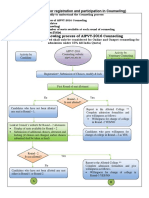
- Counseling Procedure On WebDocumento2 pagineCounseling Procedure On Webసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- User'S Manual FOR Candidates FOR: Online Registration & Choice FillingDocumento16 pagineUser'S Manual FOR Candidates FOR: Online Registration & Choice Fillingసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Frequently Asked Questions (Faqs)Documento7 pagineFrequently Asked Questions (Faqs)సాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Chronotherapeutics Handout FullDocumento2 pagineChronotherapeutics Handout Fullసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- List of Veterinary Colleges: Home AIPVT 2016 About Us Ivpr Acts, Rules and Regulations CVE Citizen Charter Contact UsDocumento4 pagineList of Veterinary Colleges: Home AIPVT 2016 About Us Ivpr Acts, Rules and Regulations CVE Citizen Charter Contact Usసాయిమహేష్రెడ్డిఆవులNessuna valutazione finora
- Эквивалентная Схема Мотра Теслы с Thomas2020Documento7 pagineЭквивалентная Схема Мотра Теслы с Thomas2020Алексей ЯмаNessuna valutazione finora
- List of Some Common Surgical TermsDocumento5 pagineList of Some Common Surgical TermsShakil MahmodNessuna valutazione finora
- Iphone and Ipad Development TU GrazDocumento2 pagineIphone and Ipad Development TU GrazMartinNessuna valutazione finora
- CS8CHP EletricalDocumento52 pagineCS8CHP EletricalCristian ricardo russoNessuna valutazione finora
- Introduction To Retail LoansDocumento2 pagineIntroduction To Retail LoansSameer ShahNessuna valutazione finora
- 1.SDH Basics PDFDocumento37 pagine1.SDH Basics PDFsafder wahabNessuna valutazione finora
- Introduction To BiogasDocumento5 pagineIntroduction To BiogasLouis EldertardNessuna valutazione finora
- Lesson Plan For Implementing NETSDocumento5 pagineLesson Plan For Implementing NETSLisa PizzutoNessuna valutazione finora
- Vemu Institute of Technology: Department of Computer Science & EngineeringDocumento79 pagineVemu Institute of Technology: Department of Computer Science & EngineeringSiva SankarNessuna valutazione finora
- EKC 202ABC ManualDocumento16 pagineEKC 202ABC ManualJose CencičNessuna valutazione finora
- WHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)Documento3 pagineWHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)114912Nessuna valutazione finora
- Feed-Pump Hydraulic Performance and Design Improvement, Phase I: J2esearch Program DesignDocumento201 pagineFeed-Pump Hydraulic Performance and Design Improvement, Phase I: J2esearch Program DesignJonasNessuna valutazione finora
- Who Trs 993 Web FinalDocumento284 pagineWho Trs 993 Web FinalAnonymous 6OPLC9UNessuna valutazione finora
- School Based INSET Interim EvaluationDocumento8 pagineSchool Based INSET Interim Evaluationprinces arcangelNessuna valutazione finora
- Organization Culture Impacts On Employee Motivation: A Case Study On An Apparel Company in Sri LankaDocumento4 pagineOrganization Culture Impacts On Employee Motivation: A Case Study On An Apparel Company in Sri LankaSupreet PurohitNessuna valutazione finora
- Ajmera - Treon - FF - R4 - 13-11-17 FinalDocumento45 pagineAjmera - Treon - FF - R4 - 13-11-17 FinalNikita KadamNessuna valutazione finora
- Grade 9 Science Biology 1 DLPDocumento13 pagineGrade 9 Science Biology 1 DLPManongdo AllanNessuna valutazione finora
- Haier in India Building Presence in A Mass Market Beyond ChinaDocumento14 pagineHaier in India Building Presence in A Mass Market Beyond ChinaGaurav Sharma100% (1)
- 5066452Documento53 pagine5066452jlcheefei9258Nessuna valutazione finora
- EKRP311 Vc-Jun2022Documento3 pagineEKRP311 Vc-Jun2022dfmosesi78Nessuna valutazione finora