Potrebbero piacerti anche
- Morgellons Disease Related To Black Magic Rituals PDFDocumento30 pagineMorgellons Disease Related To Black Magic Rituals PDFadu66680% (5)
- Fatty Liver: How To Take Care of Your LiverDocumento42 pagineFatty Liver: How To Take Care of Your Liverashrufzz90% (21)
- ABO Blood Group SystemDocumento61 pagineABO Blood Group Systemmail2jackal50% (2)
- RBC AnomaliesDocumento10 pagineRBC AnomaliesSHUPATUSSAINessuna valutazione finora
- Case Study AccretaDocumento35 pagineCase Study AccretaM Clarisse ParicoNessuna valutazione finora
- Pathophysiology Respiratory SystemDocumento63 paginePathophysiology Respiratory SystemAli Basha QudahNessuna valutazione finora
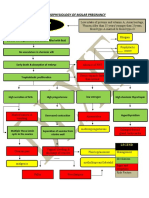
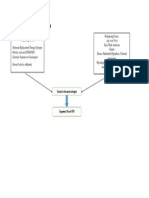
- Partial Mole or Complete Mole: Pathophysiology of Molar PregnancyDocumento1 paginaPartial Mole or Complete Mole: Pathophysiology of Molar PregnancyKristian Karl Bautista Kiw-isNessuna valutazione finora
- TIRMODDocumento66 pagineTIRMODYaniNessuna valutazione finora
- Postpartum Cesarean Section Case StudyDocumento17 paginePostpartum Cesarean Section Case StudyWeng Maesa MontemayorNessuna valutazione finora
- Anatomy and Physiology of PlacentaDocumento5 pagineAnatomy and Physiology of PlacentaAdrianne Basa100% (1)
- BSN Level III Clinical InstructorDocumento33 pagineBSN Level III Clinical InstructorChristine Bell JapitanaNessuna valutazione finora
- Ectopic PregnancyDocumento78 pagineEctopic PregnancyCarie Manarondong80% (5)
- Basics of Molecular BiologyDocumento69 pagineBasics of Molecular BiologyYasin Putra Esbeye100% (2)
- Abruptio PlacentaDocumento13 pagineAbruptio Placentamiss RN92% (12)
- PreeclampsiaDocumento58 paginePreeclampsiarhyanne100% (8)
- Pathophysiology of Uterine CancerDocumento1 paginaPathophysiology of Uterine CancerCharlotte Cordero0% (1)
- 5t4bvrfke3xuqspihwrir0d1Documento6 pagine5t4bvrfke3xuqspihwrir0d1Vishesh Mahendru20% (5)
- Incompetent CervixDocumento29 pagineIncompetent CervixCyrelle Jen TorresNessuna valutazione finora
- Placenta Previa Case StudyDocumento59 paginePlacenta Previa Case StudyKen KenNessuna valutazione finora
- Incomplete Abortion Case StudyDocumento40 pagineIncomplete Abortion Case StudyLani Michelle BelloNessuna valutazione finora
- Uterine ProlapseDocumento21 pagineUterine ProlapseFau Fau DheoboNessuna valutazione finora
- Incompetent CervixDocumento4 pagineIncompetent CervixCharm Arroyo100% (1)
- Abnormal Uterine BleedingDocumento4 pagineAbnormal Uterine BleedingAmellyn Reyes0% (1)
- Hydatidiform Mole/ Molar Pregnancy: College of Health SciencesDocumento11 pagineHydatidiform Mole/ Molar Pregnancy: College of Health SciencesAngelu Gabrielle CastroNessuna valutazione finora
- CASE STUDY On Missed AbortionDocumento5 pagineCASE STUDY On Missed AbortionOmotosho AlexNessuna valutazione finora
- 5 - Abortion or MiscarriageDocumento43 pagine5 - Abortion or Miscarriageasifdawar2011Nessuna valutazione finora
- Uterine Myoma Treatment Options for Fertility PreservationDocumento38 pagineUterine Myoma Treatment Options for Fertility PreservationErika Capitly100% (1)
- Incomplete Abortion MINI CASE STUDY (Group 3)Documento22 pagineIncomplete Abortion MINI CASE STUDY (Group 3)Twobee Evelyn Claire62% (21)
- EctopicDocumento41 pagineEctopicVillanueva Ameera MaeNessuna valutazione finora
- CP On Pre-EclampsiaDocumento152 pagineCP On Pre-Eclampsiakathy100% (2)
- A Case Study of Placenta PreviaDocumento10 pagineA Case Study of Placenta PreviaAdriane ComaNessuna valutazione finora
- Nursing Care of Hydatidiform MoleDocumento23 pagineNursing Care of Hydatidiform MoleKristel Rivamonte100% (1)
- Case Study Placenta Previa This Is It 1Documento71 pagineCase Study Placenta Previa This Is It 1Homework Ping100% (1)
- Survival in Long CaseDocumento7 pagineSurvival in Long CaseRapid MedicineNessuna valutazione finora
- Uterine MYOMADocumento5 pagineUterine MYOMARoss Manalang100% (2)
- Ectopic Pregnancy Case StudyDocumento69 pagineEctopic Pregnancy Case StudyMo-nhica Luise AlundayNessuna valutazione finora
- Case Study H MOLEDocumento11 pagineCase Study H MOLEmaori_martinez82% (11)
- Abortion CaseDocumento41 pagineAbortion Casekaycee_delacruz60% (5)
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Placenta Previa Case StudyDocumento59 paginePlacenta Previa Case StudySiergs Smith GervacioNessuna valutazione finora
- Case Study of Cesarean SectionDocumento9 pagineCase Study of Cesarean SectionErika Joy Imperio0% (1)
- Case StudyDocumento19 pagineCase Studywella goNessuna valutazione finora
- CASE ANALYSIS Ectopic Pregnancy Part 1Documento10 pagineCASE ANALYSIS Ectopic Pregnancy Part 1Diane Celine SantianoNessuna valutazione finora
- What Is Retained PlacentaDocumento7 pagineWhat Is Retained PlacentaA Xiao Yhing TrancoNessuna valutazione finora
- Endometriosis PresentationDocumento58 pagineEndometriosis PresentationBRI KUNessuna valutazione finora
- Placent Previa Case Study With Pa Tho PhysiologyDocumento6 paginePlacent Previa Case Study With Pa Tho PhysiologyRey Deemsur Salvilla MolinosNessuna valutazione finora
- Pre EclampsiaDocumento13 paginePre EclampsiaEniamrahs DnalonNessuna valutazione finora
- Case Study MiscariageDocumento14 pagineCase Study MiscariagesexiiimammaNessuna valutazione finora
- Incomplete AbortionDocumento18 pagineIncomplete AbortionAra DirganNessuna valutazione finora
- Molar Pregnancy: November 2018 Jis Dungca, Delos Santos, CrisostomoDocumento99 pagineMolar Pregnancy: November 2018 Jis Dungca, Delos Santos, CrisostomoDarnell DelgadoNessuna valutazione finora
- 35 - Retained PlacentaDocumento11 pagine35 - Retained Placentadr_asalehNessuna valutazione finora
- Case PresentationDocumento50 pagineCase Presentationapi-19762967Nessuna valutazione finora
- Case Study (Placenta Previa)Documento5 pagineCase Study (Placenta Previa)Jai - HoNessuna valutazione finora
- Nursing Care for Abruption PlacentaDocumento6 pagineNursing Care for Abruption PlacentaKrizzia Angela BacotocNessuna valutazione finora
- Casestudy Makato 2nd Pre EclampsiaDocumento7 pagineCasestudy Makato 2nd Pre EclampsiaRainier IbarretaNessuna valutazione finora
- Case Study-Cesarean BirthDocumento5 pagineCase Study-Cesarean BirthDada Malicsi Landicho100% (2)
- Sarcoma NCPDocumento8 pagineSarcoma NCPginosanNessuna valutazione finora
- Myoma Final Power PointDocumento45 pagineMyoma Final Power Pointicesexy100% (1)
- Incomplete Abortion: A Mini Case Study OnDocumento22 pagineIncomplete Abortion: A Mini Case Study OnSunny MujmuleNessuna valutazione finora
- History of Present IllnessDocumento30 pagineHistory of Present IllnessTrixia Joy R NachorNessuna valutazione finora
- A Case Study on Abnormal Uterine Bleeding and its TreatmentDocumento34 pagineA Case Study on Abnormal Uterine Bleeding and its TreatmentJervy Emiel VALENCIANessuna valutazione finora
- Case Study - Group 3 Community Health NursingDocumento31 pagineCase Study - Group 3 Community Health NursingApple MendozaNessuna valutazione finora
- ResearchDocumento12 pagineResearchHannahNessuna valutazione finora
- Abortion: Case Scenario 1Documento23 pagineAbortion: Case Scenario 1Mae Arra Lecobu-anNessuna valutazione finora
- A Case Study On Ruptured Ectopic Pregnancy: Lyceum Northwestern UniversityDocumento39 pagineA Case Study On Ruptured Ectopic Pregnancy: Lyceum Northwestern UniversityHomework PingNessuna valutazione finora
- PretermDocumento11 paginePretermAlma Gobaleza100% (2)
- Case StudyDocumento12 pagineCase StudyAllan Roy Malibiran BalderamaNessuna valutazione finora
- Evidence-Based Practice in Maternal & Child HealthDocumento15 pagineEvidence-Based Practice in Maternal & Child HealthJan Oliver YaresNessuna valutazione finora
- 37 Grand Case Manuscript 4Documento62 pagine37 Grand Case Manuscript 4Marjune DimayugaNessuna valutazione finora
- Eucerin - Nobel Prize Revolutionises Skin Care - Cells' Water Channels Specifically StimulatedDocumento2 pagineEucerin - Nobel Prize Revolutionises Skin Care - Cells' Water Channels Specifically StimulatedFelpnilNessuna valutazione finora
- EBMT 2021 ProgramDocumento288 pagineEBMT 2021 Programtirillas101Nessuna valutazione finora
- Colorectal Cancer 1Documento71 pagineColorectal Cancer 1Anupam SisodiaNessuna valutazione finora
- Upadacitinib AR SELECT NEXT TrialDocumento10 pagineUpadacitinib AR SELECT NEXT TrialMr. LNessuna valutazione finora
- M.03 Non-Mendelian GeneticsDocumento5 pagineM.03 Non-Mendelian Geneticsno veNessuna valutazione finora
- Paper de JB FRBDocumento1 paginaPaper de JB FRBjbenitesvilchezNessuna valutazione finora
- Clinical and Etiological Profile of Unprovoked Thrombosis in Young Patients Admitted at A Tertiary Care HospitalDocumento5 pagineClinical and Etiological Profile of Unprovoked Thrombosis in Young Patients Admitted at A Tertiary Care HospitalfarhanomeNessuna valutazione finora
- Tools of BioinformaticsDocumento29 pagineTools of BioinformaticsM HaroonNessuna valutazione finora
- Birth Defects and Prenatal DiagnosisDocumento49 pagineBirth Defects and Prenatal DiagnosiskurniaNessuna valutazione finora
- Thapar, Cooper, Eyre y LangleyDocumento15 pagineThapar, Cooper, Eyre y LangleyNicol Mariana V. FernándezNessuna valutazione finora
- I.-NCP John Richmond LacadenDocumento3 pagineI.-NCP John Richmond LacadenRichmond Lacaden100% (1)
- Bio All ModulesDocumento561 pagineBio All ModulesBlake M RhoadesNessuna valutazione finora
- Bayer Pharma RD Event 2023Documento135 pagineBayer Pharma RD Event 2023ranvijay.rajput515Nessuna valutazione finora
- Antinuclear AntibodiesDocumento99 pagineAntinuclear Antibodiesdudapaskas100% (1)
- 1.0 Personal Particular: CV-DR Fadzilah Adibah BT HJ Abdul Majid (UTM ID 6337)Documento29 pagine1.0 Personal Particular: CV-DR Fadzilah Adibah BT HJ Abdul Majid (UTM ID 6337)Sanmakhrozal HaqiqiNessuna valutazione finora
- Terapia Multimodal Con Vasopresores en Shock Septico 2023Documento11 pagineTerapia Multimodal Con Vasopresores en Shock Septico 2023CESAR AUGUSTO AUCCACUSI RODRIGUEZNessuna valutazione finora
- Purves Neuroscience Website Questions CH 8 AnswersDocumento4 paginePurves Neuroscience Website Questions CH 8 AnswersPK3214598750% (2)
- Dissociative Identity Disorder Research OverviewDocumento7 pagineDissociative Identity Disorder Research Overviewthom_evans_2Nessuna valutazione finora
- Antigen Processing and Presentation 09Documento34 pagineAntigen Processing and Presentation 09Khairul Ikhwan100% (2)
- Corey Dambacher, Ph.D. Recognized As A Professional of The Year by Strathmore's Who's Who Worldwide PublicationDocumento2 pagineCorey Dambacher, Ph.D. Recognized As A Professional of The Year by Strathmore's Who's Who Worldwide PublicationPR.comNessuna valutazione finora
- Imse LectureDocumento19 pagineImse LectureJOWELA RUBY EUSEBIONessuna valutazione finora