Potrebbero piacerti anche
- Spine: HistoryDocumento6 pagineSpine: HistorySham SundarNessuna valutazione finora
- Fam Med OsceDocumento5 pagineFam Med OsceNathan KimNessuna valutazione finora
- Examination of Bone and Joint PathologyDocumento89 pagineExamination of Bone and Joint PathologyMuhammad Thahir100% (1)
- Musculoskeletal SystemDocumento160 pagineMusculoskeletal SystemAirene Aquino BusaniaNessuna valutazione finora
- Shoulder Impinge MentDocumento26 pagineShoulder Impinge MentkotraeNessuna valutazione finora
- Hip and Buttock PainDocumento26 pagineHip and Buttock PainEdy SetiawanNessuna valutazione finora
- ShoulderDocumento51 pagineShoulderIts LaraNessuna valutazione finora
- Lec7 Assessment of SpineDocumento35 pagineLec7 Assessment of Spinesana mumtazNessuna valutazione finora
- Joint ExaminationsDocumento6 pagineJoint Examinationsjoelh9Nessuna valutazione finora
- Range of MotionDocumento36 pagineRange of Motiontrk_hussain100% (2)
- PT Measurement Practical-2Documento28 paginePT Measurement Practical-2Anthony PatrickNessuna valutazione finora
- Ex - Neuro ULDocumento3 pagineEx - Neuro ULssNessuna valutazione finora
- Assessment of The Musclo-Skletal SystemDocumento25 pagineAssessment of The Musclo-Skletal SystemjacnpoyNessuna valutazione finora
- Approach To ArthralgiaDocumento5 pagineApproach To ArthralgiaBlaire FultoneNessuna valutazione finora
- Musculoskeletal AssessmentDocumento69 pagineMusculoskeletal AssessmentWorku Kifle100% (2)
- Examination of The Joints and ExtremitiesDocumento66 pagineExamination of The Joints and Extremitiesapi-25914483Nessuna valutazione finora
- Assessment of The Musculo-Skeletal SystemDocumento46 pagineAssessment of The Musculo-Skeletal SystemRaquel M. MendozaNessuna valutazione finora
- Shoulder ExaminationDocumento4 pagineShoulder ExaminationYS NateNessuna valutazione finora
- Shoulder Case Study 1Documento4 pagineShoulder Case Study 1superhoofy718667% (3)
- Assessmentofshoulder 180107041721Documento36 pagineAssessmentofshoulder 180107041721Chandra PrabhaNessuna valutazione finora
- Day 2 - Back ExamDocumento20 pagineDay 2 - Back ExamTingting GeNessuna valutazione finora
- Spine ExaminationDocumento30 pagineSpine ExaminationNadia SalwaniNessuna valutazione finora
- N1J02 Week #2 Musculoskeletal Handout ROM For StudentsDocumento4 pagineN1J02 Week #2 Musculoskeletal Handout ROM For StudentsNatalie UrquhartNessuna valutazione finora
- Elbow PT AssessmentDocumento31 pagineElbow PT Assessmentkrissh20Nessuna valutazione finora
- Hip Examination - OSCE Guide - Geeky MedicsDocumento6 pagineHip Examination - OSCE Guide - Geeky MedicsAmcDelhiNessuna valutazione finora
- The Examination of The Knee - 040716Documento35 pagineThe Examination of The Knee - 040716Mufidah FidaNessuna valutazione finora
- Physical Examination of The Shoulder FinalDocumento28 paginePhysical Examination of The Shoulder FinalAndinNessuna valutazione finora
- Cervical Ortho TestsDocumento74 pagineCervical Ortho Testsjdavis3100% (1)
- Workshop PPT (Final) Knee JointDocumento127 pagineWorkshop PPT (Final) Knee Jointpasha100% (2)
- Manual Handling Presentation: Understanding Your BodyDocumento28 pagineManual Handling Presentation: Understanding Your BodyvhlactaotaoNessuna valutazione finora
- Musculoskeletal Curriculum: History & Physical Exam of The ShoulderDocumento60 pagineMusculoskeletal Curriculum: History & Physical Exam of The Shoulderhis.thunder122100% (1)
- Screenshot 2022-09-19 at 7.52.43 AMDocumento102 pagineScreenshot 2022-09-19 at 7.52.43 AMkamalesvati5Nessuna valutazione finora
- Assessment of Cervical Spine: By: Khushali Jogani The Sarvajanik College of Physiotherapy Rampura, SuratDocumento36 pagineAssessment of Cervical Spine: By: Khushali Jogani The Sarvajanik College of Physiotherapy Rampura, SuratAli ImranNessuna valutazione finora
- Physioterapy SalveDocumento45 paginePhysioterapy SalveIkhar KeliobasNessuna valutazione finora
- OADocumento8 pagineOAHengkai NeoNessuna valutazione finora
- Done By: Team Leader:: Rawan Altaleb Khulood AlraddadiDocumento6 pagineDone By: Team Leader:: Rawan Altaleb Khulood Alraddadishagufta lailaNessuna valutazione finora
- Hamstring Tendinopathy Case PresentationDocumento22 pagineHamstring Tendinopathy Case PresentationprohormusicNessuna valutazione finora
- PositioningDocumento3 paginePositioningMabesNessuna valutazione finora
- Examination of Spine: DR Thit Lwin Senior Lecturer UMSDocumento32 pagineExamination of Spine: DR Thit Lwin Senior Lecturer UMSStar CruiseNessuna valutazione finora
- Clinical Presentation 2.0Documento61 pagineClinical Presentation 2.0Danial AdliNessuna valutazione finora
- Ortho PE NotesDocumento35 pagineOrtho PE NotesSudesna Roy ChowdhuryNessuna valutazione finora
- Passive Range of Motion NursesDocumento32 paginePassive Range of Motion NurseszeinabNessuna valutazione finora
- Hip ExaminationDocumento4 pagineHip ExaminationLiyana Huda KamaruddinNessuna valutazione finora
- MSK Spine ScriptDocumento4 pagineMSK Spine ScriptRay ChangNessuna valutazione finora
- Knee PP Revision:: 1. Flexion (0 - 135)Documento13 pagineKnee PP Revision:: 1. Flexion (0 - 135)senoNessuna valutazione finora
- Examenul Clinic Al GenunchiuluiDocumento21 pagineExamenul Clinic Al GenunchiuluiPetru GanganNessuna valutazione finora
- Spondylolysis SpondylolisthesisDocumento89 pagineSpondylolysis SpondylolisthesisAh ZhangNessuna valutazione finora
- Clinical Examination of The Knee: DR John EbnezarDocumento95 pagineClinical Examination of The Knee: DR John EbnezarsandeepNessuna valutazione finora
- Examination of ElbowDocumento18 pagineExamination of Elbowharmohit singhNessuna valutazione finora
- FUNDA REVIEW 2 Body MechanicsDocumento27 pagineFUNDA REVIEW 2 Body Mechanicslovie dooNessuna valutazione finora
- MSK IV PracticalDocumento10 pagineMSK IV Practicalroshanleung11Nessuna valutazione finora
- Pemeriksaan Fisik BahuDocumento35 paginePemeriksaan Fisik BahuShone NamNessuna valutazione finora
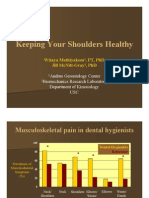
- Keeping Your Shoulders HealthyDocumento38 pagineKeeping Your Shoulders Healthyxyz84Nessuna valutazione finora
- Spine Exam 2Documento44 pagineSpine Exam 2Azmi FarhadiNessuna valutazione finora
- GALS AssessmentDocumento46 pagineGALS AssessmentdrindrasNessuna valutazione finora
- Lateral Epicondylitis: ST NDDocumento2 pagineLateral Epicondylitis: ST NDMuhammad Ucuk100% (1)
- WK 6 Study QsDocumento7 pagineWK 6 Study Qsapi-479720222Nessuna valutazione finora
- 3 Back and Joints March 2011Documento19 pagine3 Back and Joints March 2011suaqaziNessuna valutazione finora
- Mustafa CV PDFDocumento22 pagineMustafa CV PDFMUSTAFA TEMEMINessuna valutazione finora
- Practice Sheet Session 2 - 2021 - Student SheetDocumento2 paginePractice Sheet Session 2 - 2021 - Student SheetAlisa SayNessuna valutazione finora
- Acuna - ENG 2089 AAEDocumento2 pagineAcuna - ENG 2089 AAERishi GolaniNessuna valutazione finora
- How God Changes Your Brain: The Big IdeasDocumento6 pagineHow God Changes Your Brain: The Big Ideasmatache vali100% (1)
- Food Systems For ChildrenDocumento12 pagineFood Systems For ChildrenPaulin koffiNessuna valutazione finora
- Role of Forensic MedicineDocumento5 pagineRole of Forensic MedicinemkumNessuna valutazione finora
- SES Presentation FinalDocumento65 pagineSES Presentation FinalCurtis YehNessuna valutazione finora
- Q1 Health Status QuestionnaireDocumento2 pagineQ1 Health Status QuestionnaireKathleen ChuaNessuna valutazione finora
- Family and Community Profile I. General InformationDocumento4 pagineFamily and Community Profile I. General InformationMary Leour PascuaNessuna valutazione finora
- Professional Review Industry Route Guidance NotesDocumento10 pagineProfessional Review Industry Route Guidance NotesAnonymous TlYmhkNessuna valutazione finora
- Ellness F T I O: Rom He Nside UtDocumento5 pagineEllness F T I O: Rom He Nside UthbgossNessuna valutazione finora
- Lecture #3 - Carbohydrates & LipidsDocumento23 pagineLecture #3 - Carbohydrates & Lipidsogangurel100% (3)
- Craniofacial SyndromesDocumento101 pagineCraniofacial SyndromesSaranya MohanNessuna valutazione finora
- Pediatrics Rapid RevisionDocumento72 paginePediatrics Rapid RevisionWorld MedclickzNessuna valutazione finora
- Example: Write Sentences To Give Advice. Use The Verb and The Information in Parenthesis. (1.25 Points)Documento2 pagineExample: Write Sentences To Give Advice. Use The Verb and The Information in Parenthesis. (1.25 Points)Robert Jesús Guerrero GilerNessuna valutazione finora
- Combat StressDocumento94 pagineCombat StressClaudia Maria Ivan100% (1)
- QUARTER 3 WEEK 3 English For Academic and PPDocumento11 pagineQUARTER 3 WEEK 3 English For Academic and PPCharmaine PearlNessuna valutazione finora
- Topic 58 UKfrom1945Documento10 pagineTopic 58 UKfrom1945Ana Giráldez RodríguezNessuna valutazione finora
- Paper On Rag PickersDocumento11 paginePaper On Rag PickershsrapsNessuna valutazione finora
- Interval TrainingDocumento24 pagineInterval TrainingRukmantaraNessuna valutazione finora
- Summarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedDocumento9 pagineSummarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedflashjetNessuna valutazione finora
- MarriottDocumento4 pagineMarriottSheikh Farhan AliNessuna valutazione finora
- HeartDocumento12 pagineHeartRebar photographyNessuna valutazione finora
- Cervicogenic Dizziness: DefinitionDocumento9 pagineCervicogenic Dizziness: DefinitionpervinkumarNessuna valutazione finora
- Syba Economics Syll 20-21Documento13 pagineSyba Economics Syll 20-21Saniya ShaikhNessuna valutazione finora
- Handout On The Concept of Health and Health EducationDocumento5 pagineHandout On The Concept of Health and Health Educationmomo connorNessuna valutazione finora
- CHC Proposal Letter - Dominion (1) - 1Documento2 pagineCHC Proposal Letter - Dominion (1) - 1drofiliNessuna valutazione finora
- PHC Assignment 1Documento5 paginePHC Assignment 1Florenze Laiza Donor Lucas100% (1)
- UrethralstricturesDocumento37 pagineUrethralstricturesNinaNessuna valutazione finora
- The Rating Scale Is As FollowsDocumento3 pagineThe Rating Scale Is As Followscarollim1008Nessuna valutazione finora