Potrebbero piacerti anche
- Cleanliness Throughout Life: The Importance of Showering from Childhood to AdulthoodDa EverandCleanliness Throughout Life: The Importance of Showering from Childhood to AdulthoodNessuna valutazione finora
- HygieneDocumento23 pagineHygienecaitlyntreacyNessuna valutazione finora
- Hygiene PromotionDocumento9 pagineHygiene PromotionAhmad Fahim ShahiNessuna valutazione finora
- Mainstreaming Water Safety Plans in ADB Water Sector Projects: Lessons and ChallengesDa EverandMainstreaming Water Safety Plans in ADB Water Sector Projects: Lessons and ChallengesNessuna valutazione finora
- CommunityOrgnzng SlidesDocumento85 pagineCommunityOrgnzng SlidesKhatlen BagaresNessuna valutazione finora
- Nirmal Gram PuruskarDocumento5 pagineNirmal Gram PuruskardreamzaliveNessuna valutazione finora
- WASH WEBINAR Episode 2 - Hygiene Promotion in EmergenciesDocumento52 pagineWASH WEBINAR Episode 2 - Hygiene Promotion in EmergenciesZakash AdowNessuna valutazione finora
- Chapter 3Documento108 pagineChapter 3Jerrie Mae MenciasNessuna valutazione finora
- Hygiene - Introduction: ENVR 890 Mark D. Sobsey Spring, 2007Documento28 pagineHygiene - Introduction: ENVR 890 Mark D. Sobsey Spring, 2007mahe_sce4702Nessuna valutazione finora
- Wash 7Documento22 pagineWash 7mrdaauud09Nessuna valutazione finora
- Sphere Standards: Water Supply, Sanitation and Hygiene Promotion (WASH)Documento29 pagineSphere Standards: Water Supply, Sanitation and Hygiene Promotion (WASH)Sote BrilloNessuna valutazione finora
- Affordable Access To Adequate Wash FacilitiesDocumento23 pagineAffordable Access To Adequate Wash FacilitiesJoseph GichehaNessuna valutazione finora
- People Managed Environmental Sanitation BKD Raja April 2010Documento15 paginePeople Managed Environmental Sanitation BKD Raja April 2010Bkd RajaNessuna valutazione finora
- International University Sek Environmental Sanitation Ii Group ADocumento10 pagineInternational University Sek Environmental Sanitation Ii Group AVicky JimenezNessuna valutazione finora
- Mediterranean Health Journal, 1999, 5:168-176Documento6 pagineMediterranean Health Journal, 1999, 5:168-176Marz AcopNessuna valutazione finora
- Mid Exam Environmental SanitationDocumento3 pagineMid Exam Environmental SanitationAndresurya PradanaNessuna valutazione finora
- Water Sanitation Hygiene Guidelines Global Grant Funding en PDFDocumento53 pagineWater Sanitation Hygiene Guidelines Global Grant Funding en PDFcwchiascribd99Nessuna valutazione finora
- Maldives SSHE GuidelinesDocumento8 pagineMaldives SSHE GuidelinesAnup SahooNessuna valutazione finora
- Proposed Study To Assess The Environmental Sanitation Needs of Ghanaian CommunitiesDocumento20 pagineProposed Study To Assess The Environmental Sanitation Needs of Ghanaian CommunitiesRobertus Wisnu WijayaNessuna valutazione finora
- CONSERVANCYDocumento7 pagineCONSERVANCYrodgers omondiNessuna valutazione finora
- Wash in Schools and CommunitiesDocumento61 pagineWash in Schools and Communitiesदिपेश राईNessuna valutazione finora
- Report For Practical Placement From 16th Jan To 3rd March 2017Documento20 pagineReport For Practical Placement From 16th Jan To 3rd March 2017Patrick MugoNessuna valutazione finora
- A Possible Framework For NG-CARES DLI 1.4 Nutrition Sector by Josephine Ayuk PH.DDocumento33 pagineA Possible Framework For NG-CARES DLI 1.4 Nutrition Sector by Josephine Ayuk PH.DJosephine AyukNessuna valutazione finora
- Central Java and Special Region of Yogyakarta: Environmental Services ProgramDocumento2 pagineCentral Java and Special Region of Yogyakarta: Environmental Services ProgrammuhammadnainNessuna valutazione finora
- 1.sanitation Policy and The MDGsDocumento22 pagine1.sanitation Policy and The MDGssofianina05Nessuna valutazione finora
- Action Plan Based From Prioritized Problem IdentifiedDocumento12 pagineAction Plan Based From Prioritized Problem IdentifiedCristina L. JaysonNessuna valutazione finora
- Action Plan Shreya BhatDocumento5 pagineAction Plan Shreya BhatShreeya BhatNessuna valutazione finora
- Community Health RevisionDocumento25 pagineCommunity Health RevisionfxbukenyaNessuna valutazione finora
- MeasurementDocumento1 paginaMeasurementgabrielNessuna valutazione finora
- WinsDocumento31 pagineWinsKathleen Faith Blanco VergaraNessuna valutazione finora
- Group 4Documento59 pagineGroup 4Esmel Jane Cañedo PeñaflorNessuna valutazione finora
- CLTsDocumento16 pagineCLTsrodgers omondiNessuna valutazione finora
- Sustainable Development Goals No. 1: Installation of Solar Panel On Rooftop For Electricity Generation Resouces RequiredDocumento10 pagineSustainable Development Goals No. 1: Installation of Solar Panel On Rooftop For Electricity Generation Resouces Requiredrinkuamit71Nessuna valutazione finora
- Risk Midterm Nov 6Documento8 pagineRisk Midterm Nov 6Bern ConcepcionNessuna valutazione finora
- WASH in Schools PDFDocumento56 pagineWASH in Schools PDFakhilkuwar100% (2)
- Water Sanitation Group 3Documento14 pagineWater Sanitation Group 3redhokojaNessuna valutazione finora
- Health and Hygiene Promotion Best Practices and Lessons LearnedDocumento56 pagineHealth and Hygiene Promotion Best Practices and Lessons LearnedSTBM IndonesiaNessuna valutazione finora
- CHP4 - Low ResDocumento24 pagineCHP4 - Low ResJunaid ZafarNessuna valutazione finora
- NSTP 6Documento3 pagineNSTP 6ANa AntonioNessuna valutazione finora
- WORLD BANK 2007 Hygiene and Sanitation PromotionDocumento24 pagineWORLD BANK 2007 Hygiene and Sanitation PromotionmesselecwNessuna valutazione finora
- Activity 1 ObjectiveDocumento6 pagineActivity 1 ObjectiveRei Allen RodriguezNessuna valutazione finora
- Water, Sanitation and Hygiene Education in School: A Project Proposal ONDocumento10 pagineWater, Sanitation and Hygiene Education in School: A Project Proposal ONsitheeqNessuna valutazione finora
- Sustainable Rural Water, Sanitation and Hygiene Project PROPOSALDocumento13 pagineSustainable Rural Water, Sanitation and Hygiene Project PROPOSALLawrence WatssonNessuna valutazione finora
- Project Title:: An Evaluation of The WorldDocumento23 pagineProject Title:: An Evaluation of The WorldKofi AsamoahNessuna valutazione finora
- Family Nursing Care Plan (Copy)Documento3 pagineFamily Nursing Care Plan (Copy)Christine Anne RelayoNessuna valutazione finora
- Hygiene Promotion in EmergenciesDocumento4 pagineHygiene Promotion in EmergenciesBlessing KanengoniNessuna valutazione finora
- Cholera Hosp M'Documento17 pagineCholera Hosp M'sandeshNessuna valutazione finora
- Global Health Intervention Proposal Indonesias Total Sanitation Program 1Documento5 pagineGlobal Health Intervention Proposal Indonesias Total Sanitation Program 1api-549315638Nessuna valutazione finora
- Hygiene and Sanitation Are Essential To Good HealthDocumento2 pagineHygiene and Sanitation Are Essential To Good HealthCharie Mae Gaurana BarbaNessuna valutazione finora
- Community Water Supply and Sanitation (WSEE 3143) : Chapter OneDocumento20 pagineCommunity Water Supply and Sanitation (WSEE 3143) : Chapter Onejebril yusufNessuna valutazione finora
- Health Promotion StratagiesDocumento19 pagineHealth Promotion StratagiesDawud AsnakewNessuna valutazione finora
- Hvchap 9Documento8 pagineHvchap 9Ma Michelle FranciscoNessuna valutazione finora
- Indicators For Monitoring Hygiene PromotionDocumento5 pagineIndicators For Monitoring Hygiene PromotionAbdullah SharifiNessuna valutazione finora
- Community Health NursingDocumento40 pagineCommunity Health NursingSherlyn PedidaNessuna valutazione finora
- Training For Hygiene Promotion. Part 2: Useful To KnowDocumento40 pagineTraining For Hygiene Promotion. Part 2: Useful To KnowOswar Mungkasa100% (3)
- Community Health Nursing Process0Documento59 pagineCommunity Health Nursing Process0Mukul Thakur100% (1)
- Community Health Nursing Process: Dr. Maheswari JaikumarDocumento59 pagineCommunity Health Nursing Process: Dr. Maheswari JaikumarSheryl Joy Soriano100% (1)
- L3 Health EducationDocumento18 pagineL3 Health EducationBianca GeagoniaNessuna valutazione finora
- Models of Disease Prevention Strategies 1st YearDocumento64 pagineModels of Disease Prevention Strategies 1st YearM Zohaib Irshad AhmadNessuna valutazione finora
- WALLPRES ExcavationDocumento11 pagineWALLPRES ExcavationShekh Muhsen Uddin AhmedNessuna valutazione finora
- Targeted Worker Summary Report: Economically Disadvantaged Area Hours SubtotalDocumento1 paginaTargeted Worker Summary Report: Economically Disadvantaged Area Hours SubtotalShekh Muhsen Uddin AhmedNessuna valutazione finora
- Channai MetroDocumento11 pagineChannai MetroShekh Muhsen Uddin AhmedNessuna valutazione finora
- Legend For Electrical Plan: General NotesDocumento3 pagineLegend For Electrical Plan: General NotesShekh Muhsen Uddin AhmedNessuna valutazione finora
- A Time History Analysis Method-4689Documento8 pagineA Time History Analysis Method-4689Shekh Muhsen Uddin AhmedNessuna valutazione finora
- Pile DetailsDocumento1 paginaPile DetailsShekh Muhsen Uddin AhmedNessuna valutazione finora
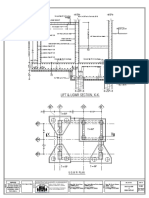
- Under Ground Reservoir DetailsDocumento1 paginaUnder Ground Reservoir DetailsShekh Muhsen Uddin AhmedNessuna valutazione finora
- b2b SpliceDocumento42 pagineb2b SpliceShekh Muhsen Uddin AhmedNessuna valutazione finora
- b2b SpliceDocumento5 pagineb2b SpliceShekh Muhsen Uddin AhmedNessuna valutazione finora
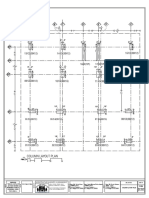
- Column Layout PlanDocumento1 paginaColumn Layout PlanShekh Muhsen Uddin Ahmed0% (1)
- Torsional Irregularity Plan ASCE 7-10 EC8Documento11 pagineTorsional Irregularity Plan ASCE 7-10 EC8Shekh Muhsen Uddin AhmedNessuna valutazione finora
- ETABS Case StudyDocumento45 pagineETABS Case StudyShekh Muhsen Uddin Ahmed100% (1)
- Materials Journal Keyword Index 2013 PDFDocumento15 pagineMaterials Journal Keyword Index 2013 PDFShekh Muhsen Uddin AhmedNessuna valutazione finora
- Pavement Design Methods 2 PDFDocumento47 paginePavement Design Methods 2 PDFShekh Muhsen Uddin AhmedNessuna valutazione finora
- Ubc 97 Type 1 Irregularity CheckDocumento11 pagineUbc 97 Type 1 Irregularity CheckShekh Muhsen Uddin AhmedNessuna valutazione finora
- ATTACH 04 - WinS Monitoring System - Blank V.2017.06.0412Documento17 pagineATTACH 04 - WinS Monitoring System - Blank V.2017.06.0412Don Mariano Marcos Elementary SchoolNessuna valutazione finora
- 117DC - Environmental Sanitation PDFDocumento8 pagine117DC - Environmental Sanitation PDFvenkiscribd444Nessuna valutazione finora
- ATP Sanitation Verification PDFDocumento2 pagineATP Sanitation Verification PDFIonuţ-Alexandru BătrînacheNessuna valutazione finora
- CE6605 Environmental Engineering IIDocumento16 pagineCE6605 Environmental Engineering IIaruNessuna valutazione finora
- EIA Report of Lai ExpresswayDocumento368 pagineEIA Report of Lai ExpresswayAbdul RehmanNessuna valutazione finora
- Draft Ordinance For Hospital WasteDocumento3 pagineDraft Ordinance For Hospital WasteGillian CalpitoNessuna valutazione finora
- Fitting Catalog 2017Documento92 pagineFitting Catalog 2017pingki04Nessuna valutazione finora
- Rights of Sanitation WorkersDocumento8 pagineRights of Sanitation Workersapi-541981758Nessuna valutazione finora
- B.Tech III Year II Semester (R13) Regular Examinations May/June 2016Documento1 paginaB.Tech III Year II Semester (R13) Regular Examinations May/June 2016Tatoo RajuNessuna valutazione finora
- Building Utilities 1 - PrelimsDocumento16 pagineBuilding Utilities 1 - PrelimsEsquibel, Mary AngelaNessuna valutazione finora
- Secondary Treatment of WastewaterDocumento19 pagineSecondary Treatment of WastewaterMary Shaniq LaurasNessuna valutazione finora
- ELDM Layout1Documento1 paginaELDM Layout1Karl Brian OdonNessuna valutazione finora
- Annual Report 2015 16Documento212 pagineAnnual Report 2015 16Telugu TamilNessuna valutazione finora
- 3 HEalth EducationDocumento23 pagine3 HEalth Educationabdullahi bashiirNessuna valutazione finora
- 19 CIVE5535 M01 S 1Documento5 pagine19 CIVE5535 M01 S 1muhammad daniyalNessuna valutazione finora
- 17.Dr Amol MinchekarDocumento12 pagine17.Dr Amol MinchekarAnonymous CwJeBCAXpNessuna valutazione finora
- COVID SDPlan BackToNormalDocumento4 pagineCOVID SDPlan BackToNormalinforumdocsNessuna valutazione finora
- Tallying Format For Community DiagnosisDocumento60 pagineTallying Format For Community DiagnosisMary Grace MendeNessuna valutazione finora
- Barangay Nutrition Scholar Action Plan, Cy 2020: BNS Form No. 2, Revised January 2018Documento9 pagineBarangay Nutrition Scholar Action Plan, Cy 2020: BNS Form No. 2, Revised January 2018Maricar Brucal EsmanaNessuna valutazione finora
- Sanitation Standard Operating Procedures: ObjectivesDocumento38 pagineSanitation Standard Operating Procedures: ObjectivesNader SedighiNessuna valutazione finora
- Methodology: Pamantasan NG Lungsod NG MaynilaDocumento3 pagineMethodology: Pamantasan NG Lungsod NG MaynilaBren SisonNessuna valutazione finora
- 'Water As This Election's Relevant (WATER) Issue'Documento12 pagine'Water As This Election's Relevant (WATER) Issue'Ralph RectoNessuna valutazione finora
- Project Management - Yamuna Action PlanDocumento13 pagineProject Management - Yamuna Action PlanSudhanshu TiwariNessuna valutazione finora
- Building System Design: 2 Semester (SY 2021-2022)Documento43 pagineBuilding System Design: 2 Semester (SY 2021-2022)Mae ManaogNessuna valutazione finora
- No. of Periods UNIT - 1: Antenna FundamentalsDocumento8 pagineNo. of Periods UNIT - 1: Antenna Fundamentalsbotla yogiNessuna valutazione finora
- Building of Mental Health Facility For People With Mental Disability Within The Vicinity of Tanauan CityDocumento5 pagineBuilding of Mental Health Facility For People With Mental Disability Within The Vicinity of Tanauan CityMutya Neri CruzNessuna valutazione finora
- Denis A Mrema: Environmental EngineerDocumento4 pagineDenis A Mrema: Environmental EngineerDennie DennyNessuna valutazione finora
- Lesson 13 Lost and Found, ETCDocumento2 pagineLesson 13 Lost and Found, ETCRoge Aronzado CabaelNessuna valutazione finora
- Dura-Blue: PVC Municipal Water Distribution Pipe (4 - 12")Documento3 pagineDura-Blue: PVC Municipal Water Distribution Pipe (4 - 12")buddhika MadusankaNessuna valutazione finora
- DM Plan Kutubdia Upazila Coxsbazar District - English Version-2014Documento89 pagineDM Plan Kutubdia Upazila Coxsbazar District - English Version-2014CDMP BangladeshNessuna valutazione finora
- Something Must Be Done About Prince Edward County: A Family, a Virginia Town, a Civil Rights BattleDa EverandSomething Must Be Done About Prince Edward County: A Family, a Virginia Town, a Civil Rights BattleValutazione: 4 su 5 stelle4/5 (34)
- When and Where I Enter: The Impact of Black Women on Race and Sex in AmericaDa EverandWhen and Where I Enter: The Impact of Black Women on Race and Sex in AmericaValutazione: 4 su 5 stelle4/5 (33)
- The War after the War: A New History of ReconstructionDa EverandThe War after the War: A New History of ReconstructionValutazione: 5 su 5 stelle5/5 (2)
- Be a Revolution: How Everyday People Are Fighting Oppression and Changing the World—and How You Can, TooDa EverandBe a Revolution: How Everyday People Are Fighting Oppression and Changing the World—and How You Can, TooValutazione: 5 su 5 stelle5/5 (2)
- Bound for Canaan: The Epic Story of the Underground Railroad, America's First Civil Rights Movement,Da EverandBound for Canaan: The Epic Story of the Underground Railroad, America's First Civil Rights Movement,Valutazione: 4.5 su 5 stelle4.5/5 (69)
- Shifting: The Double Lives of Black Women in AmericaDa EverandShifting: The Double Lives of Black Women in AmericaValutazione: 4 su 5 stelle4/5 (10)
- The Survivors of the Clotilda: The Lost Stories of the Last Captives of the American Slave TradeDa EverandThe Survivors of the Clotilda: The Lost Stories of the Last Captives of the American Slave TradeValutazione: 4.5 su 5 stelle4.5/5 (3)
- The Unprotected Class: How Anti-White Racism Is Tearing America ApartDa EverandThe Unprotected Class: How Anti-White Racism Is Tearing America ApartValutazione: 5 su 5 stelle5/5 (1)
- Say It Louder!: Black Voters, White Narratives, and Saving Our DemocracyDa EverandSay It Louder!: Black Voters, White Narratives, and Saving Our DemocracyValutazione: 4.5 su 5 stelle4.5/5 (18)
- Say It Louder!: Black Voters, White Narratives, and Saving Our DemocracyDa EverandSay It Louder!: Black Voters, White Narratives, and Saving Our DemocracyNessuna valutazione finora
- The Hidden Roots of White Supremacy: And the Path to a Shared American FutureDa EverandThe Hidden Roots of White Supremacy: And the Path to a Shared American FutureValutazione: 4 su 5 stelle4/5 (11)
- Wordslut: A Feminist Guide to Taking Back the English LanguageDa EverandWordslut: A Feminist Guide to Taking Back the English LanguageValutazione: 4.5 su 5 stelle4.5/5 (82)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesDa EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesValutazione: 5 su 5 stelle5/5 (70)
- Summary of Thomas Sowell's Social Justice FallaciesDa EverandSummary of Thomas Sowell's Social Justice FallaciesNessuna valutazione finora
- Walk Through Fire: A memoir of love, loss, and triumphDa EverandWalk Through Fire: A memoir of love, loss, and triumphValutazione: 4.5 su 5 stelle4.5/5 (72)
- Decolonizing Therapy: Oppression, Historical Trauma, and Politicizing Your PracticeDa EverandDecolonizing Therapy: Oppression, Historical Trauma, and Politicizing Your PracticeNessuna valutazione finora
- Please Stop Helping Us: How Liberals Make It Harder for Blacks to SucceedDa EverandPlease Stop Helping Us: How Liberals Make It Harder for Blacks to SucceedValutazione: 4.5 su 5 stelle4.5/5 (154)
- White Guilt: How Blacks and Whites Together Destroyed the Promise of the Civil Rights EraDa EverandWhite Guilt: How Blacks and Whites Together Destroyed the Promise of the Civil Rights EraValutazione: 4.5 su 5 stelle4.5/5 (43)
- Black Fatigue: How Racism Erodes the Mind, Body, and SpiritDa EverandBlack Fatigue: How Racism Erodes the Mind, Body, and SpiritValutazione: 4.5 su 5 stelle4.5/5 (83)
- Riot and Remembrance: The Tulsa Race War and Its LegacyDa EverandRiot and Remembrance: The Tulsa Race War and Its LegacyValutazione: 4.5 su 5 stelle4.5/5 (13)
- A Day in the Life of Abed Salama: Anatomy of a Jerusalem TragedyDa EverandA Day in the Life of Abed Salama: Anatomy of a Jerusalem TragedyValutazione: 4.5 su 5 stelle4.5/5 (19)
- Summary of Coleman Hughes's The End of Race PoliticsDa EverandSummary of Coleman Hughes's The End of Race PoliticsValutazione: 5 su 5 stelle5/5 (1)
- Shame: How America's Past Sins Have Polarized Our CountryDa EverandShame: How America's Past Sins Have Polarized Our CountryValutazione: 4.5 su 5 stelle4.5/5 (86)
- Medical Bondage: Race, Gender, and the Origins of American GynecologyDa EverandMedical Bondage: Race, Gender, and the Origins of American GynecologyValutazione: 4.5 su 5 stelle4.5/5 (75)
- Becoming All Things: How Small Changes Lead To Lasting Connections Across CulturesDa EverandBecoming All Things: How Small Changes Lead To Lasting Connections Across CulturesNessuna valutazione finora
- Not a Crime to Be Poor: The Criminalization of Poverty in AmericaDa EverandNot a Crime to Be Poor: The Criminalization of Poverty in AmericaValutazione: 4.5 su 5 stelle4.5/5 (37)