Potrebbero piacerti anche
- Palliative Care - Modul NennyDocumento31 paginePalliative Care - Modul NennyNenny Yoanitha DjalaNessuna valutazione finora
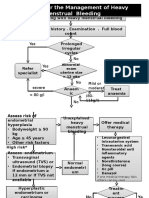
- Algorithm For The Management of Heavy Menstrual BleedingDocumento2 pagineAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNessuna valutazione finora
- Association Between MRNA Expression of Aromatase 1Documento8 pagineAssociation Between MRNA Expression of Aromatase 1Nenny Yoanitha DjalaNessuna valutazione finora
- Algorithm For The Management of Heavy Menstrual BleedingDocumento2 pagineAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNessuna valutazione finora
- Program Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Documento1 paginaProgram Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Nenny Yoanitha DjalaNessuna valutazione finora
- American Journal of Obstetrics and Gynecology Volume 207 Issue 3 2012 (Doi 10.1016/j.ajog.2012.07.031) McPherson, Jessica A. Odibo, Anthony O. Shanks, Anthony L. Ro - Impact of Chorionicity On R PDFDocumento6 pagineAmerican Journal of Obstetrics and Gynecology Volume 207 Issue 3 2012 (Doi 10.1016/j.ajog.2012.07.031) McPherson, Jessica A. Odibo, Anthony O. Shanks, Anthony L. Ro - Impact of Chorionicity On R PDFNenny Yoanitha DjalaNessuna valutazione finora
- Night Shift Duty 11 FEBRUARIDocumento2 pagineNight Shift Duty 11 FEBRUARINenny Yoanitha DjalaNessuna valutazione finora
- AJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenDocumento6 pagineAJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenNenny Yoanitha DjalaNessuna valutazione finora
- Estimated Fetal Weight Formula GuideDocumento5 pagineEstimated Fetal Weight Formula GuideNenny Yoanitha Djala100% (1)
- Medical Eligibility Criteria For Contraceptive Use Fifth Edition 2015Documento14 pagineMedical Eligibility Criteria For Contraceptive Use Fifth Edition 2015agustinasntNessuna valutazione finora
- Reichman 2014Documento5 pagineReichman 2014Nenny Yoanitha DjalaNessuna valutazione finora
- En Endometrial Cancer Guide For PatientsDocumento30 pagineEn Endometrial Cancer Guide For PatientsNenny Yoanitha DjalaNessuna valutazione finora
- Fetal and Maternal Effects of Forceps and VacuumDocumento4 pagineFetal and Maternal Effects of Forceps and VacuumNenny Yoanitha DjalaNessuna valutazione finora
- Hypertensionin PregnancyDocumento100 pagineHypertensionin Pregnancyricky hutagalungNessuna valutazione finora
- Strategi Bisnis KorporasiDocumento41 pagineStrategi Bisnis KorporasiAliMu'minHarahapNessuna valutazione finora
- Forceps Review in Modern Obstetric PracticeDocumento5 pagineForceps Review in Modern Obstetric PracticeNenny Yoanitha DjalaNessuna valutazione finora
- Termination Pregnancy Report 18 May 2010Documento45 pagineTermination Pregnancy Report 18 May 2010Nenny Yoanitha DjalaNessuna valutazione finora
- Anatomical Causes Bad Obstetric HistoryDocumento3 pagineAnatomical Causes Bad Obstetric Historykyle31Nessuna valutazione finora
- Final Data 2011 PDFDocumento90 pagineFinal Data 2011 PDFNenny Yoanitha DjalaNessuna valutazione finora
- Reichman 2014Documento5 pagineReichman 2014Nenny Yoanitha DjalaNessuna valutazione finora
- Algorithm For The Management of Heavy Menstrual BleedingDocumento2 pagineAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNessuna valutazione finora
- Obstetrical Forceps - History Mystery and MoralityDocumento16 pagineObstetrical Forceps - History Mystery and MoralityNenny Yoanitha DjalaNessuna valutazione finora
- How To Explore After Forceps ExtractionDocumento7 pagineHow To Explore After Forceps ExtractionNenny Yoanitha DjalaNessuna valutazione finora
- Forceps ExtractionDocumento49 pagineForceps ExtractionNenny Yoanitha DjalaNessuna valutazione finora
- Cytomegalovirus Infection in Patients With Active InflammatoryDocumento7 pagineCytomegalovirus Infection in Patients With Active InflammatoryNenny Yoanitha DjalaNessuna valutazione finora
- Genetic Study of TORCH Infections in Women With BOH PDFDocumento6 pagineGenetic Study of TORCH Infections in Women With BOH PDFNenny Yoanitha DjalaNessuna valutazione finora
- Reichman 2014Documento5 pagineReichman 2014Nenny Yoanitha DjalaNessuna valutazione finora
- Successful Pregnancy OutcomeDocumento6 pagineSuccessful Pregnancy OutcomeNenny Yoanitha DjalaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Checklist - A Tool For Error Management and Performance ImprovementDocumento5 pagineThe Checklist - A Tool For Error Management and Performance ImprovementGustavo Catalan RuzaNessuna valutazione finora
- Job AddendumDocumento4 pagineJob AddendumEncee MianNessuna valutazione finora
- Anterior Open BiteDocumento7 pagineAnterior Open BiteGowriNessuna valutazione finora
- Top 10 Tips For A Healthy HeartDocumento14 pagineTop 10 Tips For A Healthy HeartGiridhar AdithiyhaNessuna valutazione finora
- Lecture 24 - NSAIDsDocumento13 pagineLecture 24 - NSAIDsapi-3703352100% (1)
- NCLEX Cram SheetDocumento8 pagineNCLEX Cram SheetKaloy Kamao100% (5)
- IMMUNOHEMATOLOGY / BLOOD BANKING HISTORY AND BASICSDocumento43 pagineIMMUNOHEMATOLOGY / BLOOD BANKING HISTORY AND BASICSMarie LlanesNessuna valutazione finora
- Advance Airway MXDocumento17 pagineAdvance Airway MXMardhiyah MusaNessuna valutazione finora
- Imse Finals Reviewer - Pacate, Joyce C.Documento9 pagineImse Finals Reviewer - Pacate, Joyce C.jcpacate1178qcNessuna valutazione finora
- Top of The Foot Pain and Swelling TreatmentDocumento13 pagineTop of The Foot Pain and Swelling TreatmentNyanLinKyawNessuna valutazione finora
- Protocol - Aminoglycoside DosingDocumento5 pagineProtocol - Aminoglycoside DosingThomasNessuna valutazione finora
- Meningitis in Adults OverviewDocumento10 pagineMeningitis in Adults OverviewEmy Joy Magayanes AlcaydeNessuna valutazione finora
- Anti-Aging Effects of L-Arginine - ScienceDirectDocumento26 pagineAnti-Aging Effects of L-Arginine - ScienceDirectJohayrah DiangcaNessuna valutazione finora
- Sindromul de Tunel CarpianDocumento46 pagineSindromul de Tunel CarpianMuresan Calin100% (2)
- Argentum MettalicumDocumento11 pagineArgentum Mettalicum7477aresNessuna valutazione finora
- Epidemiology of Leprosy On Five Isolated Islands in The Flores Sea, IndonesiaDocumento9 pagineEpidemiology of Leprosy On Five Isolated Islands in The Flores Sea, IndonesiaHastuti TongkoduNessuna valutazione finora
- Effect of Cupping Massage and Modified Spinal Decompression Therapy With Exercise Therapy in Neck Radiculopathy SyndromeDocumento9 pagineEffect of Cupping Massage and Modified Spinal Decompression Therapy With Exercise Therapy in Neck Radiculopathy SyndromeKhadiga AhmadNessuna valutazione finora
- Anoxic Brain InjuryDocumento4 pagineAnoxic Brain InjuryRisky Ilona SaputraNessuna valutazione finora
- Path Anat Part 1Documento184 paginePath Anat Part 1Javier Saad100% (1)
- BIO 211 Chapter 18 Blood Assignment SummaryDocumento20 pagineBIO 211 Chapter 18 Blood Assignment Summaryf1l2o3r4e5n6Nessuna valutazione finora
- Differential DiagnosisDocumento24 pagineDifferential DiagnosisEsther EunikeNessuna valutazione finora
- 2005 Magnetom Flash 2 1Documento52 pagine2005 Magnetom Flash 2 1Herick SavioneNessuna valutazione finora
- DR Horst Filtzer AcidosisDocumento1 paginaDR Horst Filtzer AcidosisRon HipnerNessuna valutazione finora
- Urinalysis Control - Level 2 (Urnal Control 2) : Cat. No. UC5034 Lot No. 737UC Size: Expiry: 2015-10Documento6 pagineUrinalysis Control - Level 2 (Urnal Control 2) : Cat. No. UC5034 Lot No. 737UC Size: Expiry: 2015-10Meiliana ThanNessuna valutazione finora
- Scientific Journal of Neurology & NeurosurgeryDocumento5 pagineScientific Journal of Neurology & NeurosurgerySciresNessuna valutazione finora
- Periodontal Health - PDFDocumento6 paginePeriodontal Health - PDFFebri Yolanda SilabanNessuna valutazione finora
- Rhopalurus Junceus: and The Treatment of CancerDocumento17 pagineRhopalurus Junceus: and The Treatment of CancerAmalia Tri UtamiNessuna valutazione finora
- ADVANCED LIFE SUPPORT Training Manual Final 2017Documento85 pagineADVANCED LIFE SUPPORT Training Manual Final 2017Jeevan Velan94% (18)
- PlebitisDocumento2 paginePlebitiscyclops09100% (2)
- CCRISP 3rd Ed Care of Critically Sick PatientDocumento273 pagineCCRISP 3rd Ed Care of Critically Sick Patientmoh93% (14)