Potrebbero piacerti anche
- THE HELMINTHS: KEY PARASITIC WORMSDocumento9 pagineTHE HELMINTHS: KEY PARASITIC WORMSMomo ShinNessuna valutazione finora
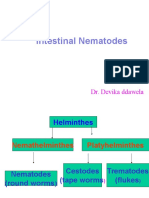
- Intestinal Nematodes: Dr. Devika DdawelaDocumento127 pagineIntestinal Nematodes: Dr. Devika DdawelaPraveenKumarNessuna valutazione finora
- INTESTINAL NEMATODES Hand Out 10 - 11Documento6 pagineINTESTINAL NEMATODES Hand Out 10 - 11microperadeniyaNessuna valutazione finora
- Parasitology Lecture 11 - AphasmidsDocumento4 pagineParasitology Lecture 11 - Aphasmidsmiguel cuevasNessuna valutazione finora
- Unit - Three: HelminthsDocumento177 pagineUnit - Three: HelminthsDembalu NuguseNessuna valutazione finora
- Intestinal RoundwormsDocumento16 pagineIntestinal RoundwormsEnaWahahaNessuna valutazione finora
- Revision: Types of Life Cycle in Trematoda and CestodaDocumento71 pagineRevision: Types of Life Cycle in Trematoda and CestodaMicroscopeGeekNessuna valutazione finora
- Ascaris LumbricoidesDocumento33 pagineAscaris LumbricoidesRosi Gustina100% (5)
- Trematoda UsusDocumento38 pagineTrematoda Ususdevi nurdiantiNessuna valutazione finora
- Nematode Infections 2019 Student PDFDocumento272 pagineNematode Infections 2019 Student PDFCharlene SuliganNessuna valutazione finora
- Trem-Ing pptIIDocumento61 pagineTrem-Ing pptIITutde SedanaNessuna valutazione finora
- Causal Agent:: Alien Invasion 1) Trichuriasis World-Wide Distribution It Is The Third Most Common Worm of ManDocumento12 pagineCausal Agent:: Alien Invasion 1) Trichuriasis World-Wide Distribution It Is The Third Most Common Worm of ManLee Zheng CongNessuna valutazione finora
- Taenia SoliumDocumento44 pagineTaenia SoliumRanti AgustiniNessuna valutazione finora
- Ascaris LumbricoidesDocumento33 pagineAscaris LumbricoidesBio SciencesNessuna valutazione finora
- Ascaris Lumbricoides: Ascariasis. Infections Most Often Seen in Young Children byDocumento7 pagineAscaris Lumbricoides: Ascariasis. Infections Most Often Seen in Young Children byThea GonzalesNessuna valutazione finora
- AscariasisDocumento44 pagineAscariasisMuhammad AuliaNessuna valutazione finora
- Common Helminthic Infections: Symptoms, Life Cycles and TreatmentDocumento63 pagineCommon Helminthic Infections: Symptoms, Life Cycles and TreatmentRafif AmirNessuna valutazione finora
- Roundworms: Characteristics, Types & DiseasesDocumento257 pagineRoundworms: Characteristics, Types & Diseasessummer dj100% (1)
- Platyhelminthes: Hazel Anne L. Tabo Olgga A. HaraDocumento79 paginePlatyhelminthes: Hazel Anne L. Tabo Olgga A. HaraHara OgheeNessuna valutazione finora
- Helminths: NematodesDocumento17 pagineHelminths: NematodesNicolle PanchoNessuna valutazione finora
- Outline: 1. General Characteristics of Platyhelminthes 2. Classification of Platyhelminthes 3. Cestodes 4. TrematodesDocumento73 pagineOutline: 1. General Characteristics of Platyhelminthes 2. Classification of Platyhelminthes 3. Cestodes 4. TrematodesAsxe CeeNessuna valutazione finora
- Ces TodosDocumento20 pagineCes TodosRudEcita RudyNessuna valutazione finora
- Trichinella and TrichurisDocumento36 pagineTrichinella and TrichurisCristine BarrozaNessuna valutazione finora
- Ascaris LumbricoidesDocumento15 pagineAscaris LumbricoidesJyoti DasNessuna valutazione finora
- Cestodes Trematodes: Agustina Tri Endharti Ssi.,Ph.DDocumento42 pagineCestodes Trematodes: Agustina Tri Endharti Ssi.,Ph.DAndre_rarungNessuna valutazione finora
- Cestode SDocumento79 pagineCestode SVincent Manganaan67% (3)
- Knowledge ReviewDocumento81 pagineKnowledge ReviewAmr EldemardashNessuna valutazione finora
- Granulosus and E. Multilocularis (Hydatid) .: Tenia Solium or T. Saginata (Teniasis)Documento7 pagineGranulosus and E. Multilocularis (Hydatid) .: Tenia Solium or T. Saginata (Teniasis)moosNessuna valutazione finora
- AscarisDocumento3 pagineAscarisColette BarrometroNessuna valutazione finora
- Schistopresentation 150629172317 Lva1 App6891Documento43 pagineSchistopresentation 150629172317 Lva1 App6891Briana NdayisabaNessuna valutazione finora
- Kuliah Cacing WestyDocumento63 pagineKuliah Cacing WestyIndra ToshiwayNessuna valutazione finora
- Nematodes 10-11Documento128 pagineNematodes 10-11microperadeniya100% (4)
- Phylum NematodaDocumento285 paginePhylum NematodaBrielleNessuna valutazione finora
- PARASITOLOGYDocumento57 paginePARASITOLOGYChellie GualbertoNessuna valutazione finora
- Module 33 Ascariasis EditedDocumento10 pagineModule 33 Ascariasis EditedPrincess Mae Sierra PacificoNessuna valutazione finora
- whipworm 11 _(4)_.pdf - 2023.04.17 - 06.16.03pmDocumento5 paginewhipworm 11 _(4)_.pdf - 2023.04.17 - 06.16.03pmHussainNessuna valutazione finora
- Para-Transes Prelim Exam - Unit 2Documento20 paginePara-Transes Prelim Exam - Unit 2Aysha AishaNessuna valutazione finora
- Ascaris Lumbricoides: MorphologyDocumento7 pagineAscaris Lumbricoides: MorphologyIntan HaddadNessuna valutazione finora
- Ronald G. Daroya, M.DDocumento72 pagineRonald G. Daroya, M.DJhenestka Joy SorianoNessuna valutazione finora
- Handouts Avian Salmonellosis Fall 2020Documento8 pagineHandouts Avian Salmonellosis Fall 2020NabeelNessuna valutazione finora
- Intestinal Parasitism: ProtozoansDocumento10 pagineIntestinal Parasitism: ProtozoansdtimtimanNessuna valutazione finora
- Ascaris Lumbricoides: I. MorphologyDocumento6 pagineAscaris Lumbricoides: I. MorphologyJoseline SorianoNessuna valutazione finora
- Ascariasis Ada Gambar 2Documento4 pagineAscariasis Ada Gambar 2ninaNessuna valutazione finora
- Nematodes NotesDocumento9 pagineNematodes NotesAlbert AlegreNessuna valutazione finora
- Parasaitology HelminthDocumento139 pagineParasaitology Helminthkidus asnNessuna valutazione finora
- CoccidiosisDocumento88 pagineCoccidiosisVenkatapradeepNessuna valutazione finora
- RingwormsDocumento5 pagineRingwormsCitrusNessuna valutazione finora
- The NematodesDocumento6 pagineThe NematodesVirginia ChanNessuna valutazione finora
- Hymenolepis Nana Group 5 Write UpDocumento7 pagineHymenolepis Nana Group 5 Write UpSusan GachukiaNessuna valutazione finora
- Diphyllobothrium Latum: Morphology (Adults)Documento11 pagineDiphyllobothrium Latum: Morphology (Adults)Sheana TmplNessuna valutazione finora
- Medical Biology 6Documento58 pagineMedical Biology 6Yusuf Yağız TimurNessuna valutazione finora
- Luminal Protozoan Infections of the Gastrointestinal TractDocumento68 pagineLuminal Protozoan Infections of the Gastrointestinal TractHeni Tri RahmawatiNessuna valutazione finora
- Aljas&Bama (Microbm9evaluate)Documento8 pagineAljas&Bama (Microbm9evaluate)Mary Clare Fuentes BamaNessuna valutazione finora
- NematodaDocumento96 pagineNematodaPurplesmilezNessuna valutazione finora
- Nematodes Infections of The IntestineDocumento17 pagineNematodes Infections of The Intestineabcde990075Nessuna valutazione finora
- 911 Pigeon Disease & Treatment Protocols!Da Everand911 Pigeon Disease & Treatment Protocols!Valutazione: 4 su 5 stelle4/5 (1)
- Cisitcercosis: enfermedad parasitariaDa EverandCisitcercosis: enfermedad parasitariaNessuna valutazione finora
- Computer ModuleDocumento8 pagineComputer ModuleJayricDepalobosNessuna valutazione finora
- The LightDocumento2 pagineThe LightJayricDepalobosNessuna valutazione finora
- Shipping Confirmation 1264941Documento1 paginaShipping Confirmation 1264941JayricDepalobosNessuna valutazione finora
- FWD: Schedule Change AdvisoryDocumento2 pagineFWD: Schedule Change AdvisoryJayricDepalobosNessuna valutazione finora
- Chapter 01 ChoicesDocumento9 pagineChapter 01 ChoicesJayricDepalobosNessuna valutazione finora
- WWW SlidDocumento1 paginaWWW SlidJayricDepalobosNessuna valutazione finora
- Conjunctivitis (Inclusion) Vs Acute Bacterial ConjunctivitisDocumento13 pagineConjunctivitis (Inclusion) Vs Acute Bacterial ConjunctivitisJayricDepalobosNessuna valutazione finora
- Music Order for Northern Luzon Adventist CollegeDocumento1 paginaMusic Order for Northern Luzon Adventist CollegeJayricDepalobosNessuna valutazione finora
- Conjunctivitis (Inclusion) Vs Acute Bacterial ConjunctivitisDocumento13 pagineConjunctivitis (Inclusion) Vs Acute Bacterial ConjunctivitisJayricDepalobosNessuna valutazione finora
- FWD: Schedule Change AdvisoryDocumento2 pagineFWD: Schedule Change AdvisoryJayricDepalobosNessuna valutazione finora
- Medical Ward 1 Service 2 CensusDocumento13 pagineMedical Ward 1 Service 2 CensusJayricDepalobosNessuna valutazione finora
- Sample Child Dedication ProgramDocumento1 paginaSample Child Dedication ProgramJayricDepalobos100% (2)
- The Church Must Stand TogetherDocumento7 pagineThe Church Must Stand TogetherJayricDepalobosNessuna valutazione finora
- Conjunctivitis (Inclusion) Vs Acute Bacterial ConjunctivitisDocumento13 pagineConjunctivitis (Inclusion) Vs Acute Bacterial ConjunctivitisJayricDepalobosNessuna valutazione finora
- Medical Ward 1 Service 2 CensusDocumento13 pagineMedical Ward 1 Service 2 CensusJayricDepalobosNessuna valutazione finora
- What's in A Birthday?: I. We Can Be Mixed Blessings To OthersDocumento2 pagineWhat's in A Birthday?: I. We Can Be Mixed Blessings To OthersJayricDepalobosNessuna valutazione finora
- Acquaintance Party ParticipantsDocumento1 paginaAcquaintance Party ParticipantsJayricDepalobosNessuna valutazione finora
- "Better Is The Day of Death": Feasting: For That Is The End of All Men and The Living Will Lay It To His Heart."Documento3 pagine"Better Is The Day of Death": Feasting: For That Is The End of All Men and The Living Will Lay It To His Heart."JayricDepalobosNessuna valutazione finora
- YHH Strategic Plan 2016-2017Documento5 pagineYHH Strategic Plan 2016-2017JayricDepalobosNessuna valutazione finora
- Clinical Pastoral OrientationDocumento3 pagineClinical Pastoral OrientationJayricDepalobos100% (1)
- General Anesthesia in Caesarean SectionDocumento7 pagineGeneral Anesthesia in Caesarean SectionJayricDepalobosNessuna valutazione finora
- CAA Concert ProgramDocumento2 pagineCAA Concert ProgramJayricDepalobosNessuna valutazione finora
- Census TemplateDocumento3 pagineCensus TemplateJayricDepalobosNessuna valutazione finora
- Psalm 23 SermonDocumento5 paginePsalm 23 SermonJayricDepalobosNessuna valutazione finora
- Tally Sheeth Per 10 HouseholdsDocumento14 pagineTally Sheeth Per 10 HouseholdsJayricDepalobosNessuna valutazione finora
- Teen Parenting Brochure AssignmentDocumento1 paginaTeen Parenting Brochure AssignmentJayricDepalobosNessuna valutazione finora
- Understanding Thalassemia: Causes, Symptoms and TreatmentDocumento19 pagineUnderstanding Thalassemia: Causes, Symptoms and TreatmentJayricDepalobosNessuna valutazione finora
- Peer Evaluation For Group 5Documento1 paginaPeer Evaluation For Group 5JayricDepalobosNessuna valutazione finora
- Tally Sheeth Per 10 HouseholdsDocumento14 pagineTally Sheeth Per 10 HouseholdsJayricDepalobosNessuna valutazione finora
- Pneumonia Antibiotics PDFDocumento1 paginaPneumonia Antibiotics PDFRudy KurniawanNessuna valutazione finora
- Lesson 4 - Circulatory SystemDocumento21 pagineLesson 4 - Circulatory SystemJoseeNessuna valutazione finora
- Male and Female Sexual Dysfunction-072343266XDocumento287 pagineMale and Female Sexual Dysfunction-072343266XLikoh Timothy100% (2)
- HipertiroidDocumento37 pagineHipertiroidTaysqy swftNessuna valutazione finora
- Female Repro Part1 - GomezDocumento27 pagineFemale Repro Part1 - GomezMelissa SalayogNessuna valutazione finora
- Prevalence of Crossbite in Primary DentitionDocumento4 paginePrevalence of Crossbite in Primary DentitionSilvia Marcela RojasNessuna valutazione finora
- Anatomy and Physiology Chapter11 The Muscular SystemDocumento18 pagineAnatomy and Physiology Chapter11 The Muscular SystemDayledaniel SorvetoNessuna valutazione finora
- Biology Essay Questions Expected Answers PDFDocumento31 pagineBiology Essay Questions Expected Answers PDFAlexander Kinyoda100% (1)
- Anatomy of The Liver and Biliary SystemDocumento11 pagineAnatomy of The Liver and Biliary Systemapi-372329083% (6)
- Mcqs - Biochemistry - Immune Response - PFMSG ForumDocumento4 pagineMcqs - Biochemistry - Immune Response - PFMSG ForumDillu SahuNessuna valutazione finora
- Alat Lab Di IkmDocumento20 pagineAlat Lab Di Ikmnur hasanahNessuna valutazione finora
- Quick Review PDFDocumento154 pagineQuick Review PDFDr PenCaster100% (1)
- Anatomy and Pathophysiology of ProstrateDocumento44 pagineAnatomy and Pathophysiology of Prostraterajan kumar100% (3)
- Immunology Qs - Part #3, M.TawalbehDocumento16 pagineImmunology Qs - Part #3, M.TawalbehMohamed Tawalbe100% (3)
- Iron Deficiency AnemiaDocumento12 pagineIron Deficiency AnemiaAnkush GahlotNessuna valutazione finora
- CVS1 - K3. Fungsi Sistem KardiovaskularDocumento20 pagineCVS1 - K3. Fungsi Sistem KardiovaskularsnorlaxNessuna valutazione finora
- Identifying Normal Mandibular Anatomy in Intraoral RadiographsDocumento23 pagineIdentifying Normal Mandibular Anatomy in Intraoral RadiographsPatricia SnowdenNessuna valutazione finora
- Book 1Documento6 pagineBook 1Kieth Garcia DariaNessuna valutazione finora
- Blood Trasnfusions 1Documento7 pagineBlood Trasnfusions 1Silvia RodríguezNessuna valutazione finora
- Noor Saba' PDFDocumento2 pagineNoor Saba' PDFAmresh VermaNessuna valutazione finora
- General Exam ChecklistDocumento9 pagineGeneral Exam ChecklistCodillia CheongNessuna valutazione finora
- Dopamine NeurotransmitterDocumento3 pagineDopamine NeurotransmitterPrabha Amandari SutyandiNessuna valutazione finora
- SympatheticDocumento10 pagineSympatheticSharneeshriyaNessuna valutazione finora
- 5 Functions of The Urinary SystemDocumento36 pagine5 Functions of The Urinary SystemLove Jovellanos ÜNessuna valutazione finora
- DIURETICSDocumento2 pagineDIURETICSLaureece Salm ApduhanNessuna valutazione finora
- The Endocrine SystemDocumento24 pagineThe Endocrine System속강대Nessuna valutazione finora
- Elements of Informed Consent For Blood and Blood ProductsDocumento2 pagineElements of Informed Consent For Blood and Blood ProductsKarl RobleNessuna valutazione finora
- Cap. 01 - Amphibian Anatomy and PhysiologyDocumento12 pagineCap. 01 - Amphibian Anatomy and PhysiologyNailson JúniorNessuna valutazione finora
- Anatomy Krueger April2009Documento18 pagineAnatomy Krueger April2009mele420Nessuna valutazione finora
- Reflex ArcDocumento16 pagineReflex ArcNiaz Ahammed50% (2)
- Butterfly OpusDocumento9 pagineButterfly OpusnhasuonlineNessuna valutazione finora