Potrebbero piacerti anche
- ED From The Mental Health PT Perspective - Clarke2007Documento6 pagineED From The Mental Health PT Perspective - Clarke2007Deanne Morris-DeveauxNessuna valutazione finora
- Lecture Title: Psychiatry IiDocumento1 paginaLecture Title: Psychiatry IiMiguel DomingoNessuna valutazione finora
- Psychiatric Care in The Emergency Depar Tment-Chaos or Crisis?Documento3 paginePsychiatric Care in The Emergency Depar Tment-Chaos or Crisis?dahlia4Nessuna valutazione finora
- Psychiatric EmergencyDocumento7 paginePsychiatric EmergencySiti TiaraNessuna valutazione finora
- Treatment of Ischaemic Heart Disease and Stroke in Individuals With Psychosis Under Universal HealthcareDocumento6 pagineTreatment of Ischaemic Heart Disease and Stroke in Individuals With Psychosis Under Universal Healthcareanthony.teggNessuna valutazione finora
- Approach To Consultation Psychiatry: Assessment Strategies: John Querques, M.D. Theodore A. Stern, M.DDocumento8 pagineApproach To Consultation Psychiatry: Assessment Strategies: John Querques, M.D. Theodore A. Stern, M.DDaniel MartinezNessuna valutazione finora
- Emergency Psychiatry: Care in Special SettingsDocumento15 pagineEmergency Psychiatry: Care in Special SettingsCassandra BoduchNessuna valutazione finora
- Linnen Et Al. (2011) - Depression and Essential Health Risk Factors in Surgical Patients in The Preoperative Anaesthesiological Assessment ClinicDocumento9 pagineLinnen Et Al. (2011) - Depression and Essential Health Risk Factors in Surgical Patients in The Preoperative Anaesthesiological Assessment Clinicfabienne czechNessuna valutazione finora
- 69605-Article Text-146442-1-10-20110914Documento11 pagine69605-Article Text-146442-1-10-20110914Pan PanNessuna valutazione finora
- Evaluation of A Stroke Family Care Worker Results of A Randomiset Controlled TrialDocumento23 pagineEvaluation of A Stroke Family Care Worker Results of A Randomiset Controlled TrialaNessuna valutazione finora
- Strokeaha 116 011309Documento7 pagineStrokeaha 116 011309Anvesh JallapallyNessuna valutazione finora
- Kaplan Community EpidemDocumento3 pagineKaplan Community Epidemapi-3704562Nessuna valutazione finora
- Patients' Perceptions of Care and Safety Within Psychiatric SettingsDocumento9 paginePatients' Perceptions of Care and Safety Within Psychiatric SettingsMilton MurilloNessuna valutazione finora
- Heart Failure Support Service Makes A Positive Difference: by Rebecca Ward, RNDocumento2 pagineHeart Failure Support Service Makes A Positive Difference: by Rebecca Ward, RNacma2010Nessuna valutazione finora
- Zeller Pri Psy ProofDocumento8 pagineZeller Pri Psy ProofImaNessuna valutazione finora
- Chapter 1 - Foundations of Psychiatric - Mental Health NursingDocumento5 pagineChapter 1 - Foundations of Psychiatric - Mental Health NursingCatia Fernandes100% (2)
- Hyman, Diagnosis of Mental DisordersDocumento27 pagineHyman, Diagnosis of Mental Disordersrachel.avivNessuna valutazione finora
- Decision Making C Eth Vs MDDocumento4 pagineDecision Making C Eth Vs MDLaura ValeroNessuna valutazione finora
- The Doctor's Oldest Tool: PerspectiveDocumento3 pagineThe Doctor's Oldest Tool: PerspectivePierre PradelNessuna valutazione finora
- NCM 117 Psychiatric Nursing MODULE 3Documento13 pagineNCM 117 Psychiatric Nursing MODULE 3Meryville JacildoNessuna valutazione finora
- The Psychiatric Interview in Clinical Practice - (18 The Hospitalized Patient)Documento16 pagineThe Psychiatric Interview in Clinical Practice - (18 The Hospitalized Patient)Mateus MazzaferroNessuna valutazione finora
- 1 s2.0 S0003999320303841 MainDocumento9 pagine1 s2.0 S0003999320303841 MainAFRIDATUS SAFIRANessuna valutazione finora
- Screenshot 2021-10-18 at 09.44.27Documento39 pagineScreenshot 2021-10-18 at 09.44.27Wa Ode Yulianti Asrar JayaNessuna valutazione finora
- When Psychiatric Symptoms Re Ect Medical Conditions: Authors: Killian A WelchDocumento8 pagineWhen Psychiatric Symptoms Re Ect Medical Conditions: Authors: Killian A WelchEkachaeryanti ZainNessuna valutazione finora
- Engel (1977) Need New Medical Model Challenge BiomedicineDocumento9 pagineEngel (1977) Need New Medical Model Challenge BiomedicineShawn A. WygantNessuna valutazione finora
- The Luckiest People On Earth?: PsychiatristsDocumento39 pagineThe Luckiest People On Earth?: Psychiatristsأيهم غزالNessuna valutazione finora
- International Journal of Law and Psychiatry: EditorialDocumento3 pagineInternational Journal of Law and Psychiatry: EditorialAndreea Georgiana IonescuNessuna valutazione finora
- Mental Health Nursing and First Episode PsychosisDocumento18 pagineMental Health Nursing and First Episode PsychosisleticiaNessuna valutazione finora
- Mental Health Services in CubaDocumento4 pagineMental Health Services in CubaKevin HancockNessuna valutazione finora
- Clinical Policy: Critical Issues in The Diagnosis and Management of The Adult Psychiatric Patient in The Emergency DepartmentDocumento19 pagineClinical Policy: Critical Issues in The Diagnosis and Management of The Adult Psychiatric Patient in The Emergency Departmentedurne19907249Nessuna valutazione finora
- Brakoulias, 2021 Intervencion TempranaDocumento3 pagineBrakoulias, 2021 Intervencion TempranaManuelaMartinezNessuna valutazione finora
- Mental Health Studyguide Part 1Documento39 pagineMental Health Studyguide Part 1Ngoc TB VoNessuna valutazione finora
- Brissos 2007Documento1 paginaBrissos 2007kosikevinonuNessuna valutazione finora
- Spiritual Well-Being, Depression, and Stress Among Hemodialysis Patients in JordanDocumento12 pagineSpiritual Well-Being, Depression, and Stress Among Hemodialysis Patients in JordanpangaribuansantaNessuna valutazione finora
- Dealing With Mental Disorder in PrisonersDocumento2 pagineDealing With Mental Disorder in PrisonersTaufik Muhammad JrNessuna valutazione finora
- Reversion From Mild Cognitive Impairment To Normal or Near-Normal CognitionDocumento10 pagineReversion From Mild Cognitive Impairment To Normal or Near-Normal Cognitionmadalena limaNessuna valutazione finora
- Patients With Psychiatric Disorders: What The General Dental Practitioner Needs To KnowDocumento6 paginePatients With Psychiatric Disorders: What The General Dental Practitioner Needs To KnowXavier AltamiranoNessuna valutazione finora
- Jurnal Keperawatan Jiwa Bahasa Inggris 1Documento12 pagineJurnal Keperawatan Jiwa Bahasa Inggris 1Fitry WahyuniiNessuna valutazione finora
- Spiritual PsychotherapyDocumento9 pagineSpiritual PsychotherapyDanielMartinDomingueNessuna valutazione finora
- PSYCH 001 Psychiatric Interview of The Medically Ill PDFDocumento10 paginePSYCH 001 Psychiatric Interview of The Medically Ill PDFKaye Nee100% (1)
- Psychiatric NursingDocumento20 paginePsychiatric Nursingchio0809100% (4)
- DSM5 and ICD (New)Documento10 pagineDSM5 and ICD (New)Gwen MendozaNessuna valutazione finora
- Mental Health Clinical Nurse SpecialistDocumento6 pagineMental Health Clinical Nurse Specialistapi-532618523Nessuna valutazione finora
- EmergencyDepartmentCare of ThePatientwithSuicidal OrHomicidal SymptomsDocumento10 pagineEmergencyDepartmentCare of ThePatientwithSuicidal OrHomicidal SymptomsAlfredo PreciadoNessuna valutazione finora
- Antisocial Personality DisorderDocumento12 pagineAntisocial Personality DisorderMaría Isabel Trujillo MayaNessuna valutazione finora
- Psychiatric NursingDocumento20 paginePsychiatric Nursingjohn denver floresNessuna valutazione finora
- Entrenamiento en Medicina para Residentes de PsiquiatríaDocumento3 pagineEntrenamiento en Medicina para Residentes de PsiquiatríapsychforallNessuna valutazione finora
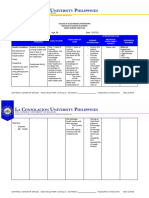
- LCUP Family Nursing Care Plan Format 2023Documento2 pagineLCUP Family Nursing Care Plan Format 2023Kia MadineNessuna valutazione finora
- Emotional Outcomes After Stroke: Factors Associated With Poor OutcomeDocumento6 pagineEmotional Outcomes After Stroke: Factors Associated With Poor OutcomeHasan KhawaldehNessuna valutazione finora
- Family Mental Health NursingDocumento21 pagineFamily Mental Health Nursinghyunra kimNessuna valutazione finora
- Nursing Diagnosis2019-2020Documento49 pagineNursing Diagnosis2019-2020Ivan MoralesNessuna valutazione finora
- Mental Health in The Philippines Status and ChallengesDocumento16 pagineMental Health in The Philippines Status and ChallengesErika BalaniNessuna valutazione finora
- Issues and ChallengesDocumento16 pagineIssues and ChallengesAriane Isshi MacatumbasNessuna valutazione finora
- Current: Don't Be Fooled by HypochondriaDocumento6 pagineCurrent: Don't Be Fooled by HypochondriaNikita UmalkarNessuna valutazione finora
- Journal of Critical Care: Bastian Matt, Daniel Schwarzkopf, Konrad Reinhart, Christian König, Christiane S. HartogDocumento6 pagineJournal of Critical Care: Bastian Matt, Daniel Schwarzkopf, Konrad Reinhart, Christian König, Christiane S. HartogPriscila FreitasNessuna valutazione finora
- Palliative CareDocumento9 paginePalliative CareJay DNessuna valutazione finora
- The Management of Psychiatric Emergencies: MedicineDocumento9 pagineThe Management of Psychiatric Emergencies: MedicineAnggi CalapiNessuna valutazione finora
- Zhou 2020 The Role of Telehealth in Reducing The Mental Health BurdenDocumento3 pagineZhou 2020 The Role of Telehealth in Reducing The Mental Health BurdenDanielaLealNessuna valutazione finora
- 2012 V 9 I 4 A 1Documento3 pagine2012 V 9 I 4 A 1acma2010Nessuna valutazione finora
- Developing A Palliative Care Service: One Hospital's ExperienceDocumento2 pagineDeveloping A Palliative Care Service: One Hospital's Experienceacma2010Nessuna valutazione finora
- 2010 V 8 I 3 A 3Documento3 pagine2010 V 8 I 3 A 3acma2010Nessuna valutazione finora
- 2010 V 8 I 2 A 1Documento3 pagine2010 V 8 I 2 A 1acma2010Nessuna valutazione finora
- 2010 V 8 I 2 A 3Documento3 pagine2010 V 8 I 2 A 3acma2010Nessuna valutazione finora
- Getting The Most From Consultant Resources: by Martha J. Koen, ACM, MN, RNDocumento2 pagineGetting The Most From Consultant Resources: by Martha J. Koen, ACM, MN, RNacma2010Nessuna valutazione finora
- Extending Care Beyond Hospital Walls: Follow-Up Program Impacts Patients and Addresses Post-Discharge NeedsDocumento3 pagineExtending Care Beyond Hospital Walls: Follow-Up Program Impacts Patients and Addresses Post-Discharge Needsacma2010Nessuna valutazione finora
- 2010 V 8 I 2 A 1Documento3 pagine2010 V 8 I 2 A 1acma2010Nessuna valutazione finora
- A Medical Director's PerspectiveDocumento4 pagineA Medical Director's Perspectiveacma2010Nessuna valutazione finora
- Opening The Door To Timely and Informative DischargeDocumento3 pagineOpening The Door To Timely and Informative Dischargeacma2010Nessuna valutazione finora
- 2010 V 8 I 3 A 3Documento3 pagine2010 V 8 I 3 A 3acma2010Nessuna valutazione finora
- 2005 V 3 I 2 A 3Documento2 pagine2005 V 3 I 2 A 3acma2010Nessuna valutazione finora
- 2003 V 1 I 3 A 1Documento2 pagine2003 V 1 I 3 A 1acma2010Nessuna valutazione finora
- My Magnificent Seven' - How Case Management Assistants Turbo-Charge The Case Management FunctionDocumento2 pagineMy Magnificent Seven' - How Case Management Assistants Turbo-Charge The Case Management Functionacma2010Nessuna valutazione finora
- 2004 V 2 I 2 A 2Documento3 pagine2004 V 2 I 2 A 2acma2010Nessuna valutazione finora
- 2004 V 2 I 2 A 1Documento2 pagine2004 V 2 I 2 A 1acma2010Nessuna valutazione finora
- 2004 V 1 I 4 A 1Documento3 pagine2004 V 1 I 4 A 1acma2010Nessuna valutazione finora
- 2003 V 1 I 3 A 3Documento2 pagine2003 V 1 I 3 A 3acma2010Nessuna valutazione finora
- A Management Engineering Approach To Improving Throughput and Shortening Overall LOS: An Unique Model For Efficiency and Time StudyDocumento2 pagineA Management Engineering Approach To Improving Throughput and Shortening Overall LOS: An Unique Model For Efficiency and Time Studyacma2010Nessuna valutazione finora
- Managing The Capacity Crisis - A Physician Advisor's PerspectiveDocumento2 pagineManaging The Capacity Crisis - A Physician Advisor's Perspectiveacma2010Nessuna valutazione finora
- 2004 V 2 I 1 A 1Documento1 pagina2004 V 2 I 1 A 1acma2010Nessuna valutazione finora
- 2004 V 2 I 2 A 3Documento2 pagine2004 V 2 I 2 A 3acma2010Nessuna valutazione finora
- Discharge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge InstructionsDocumento2 pagineDischarge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge Instructionsacma2010Nessuna valutazione finora
- 2004 V 2 I 1 A 4Documento2 pagine2004 V 2 I 1 A 4acma2010Nessuna valutazione finora
- Oncology Case Management Across The Continuum of Care: by Amelia Williams, MSWDocumento2 pagineOncology Case Management Across The Continuum of Care: by Amelia Williams, MSWacma2010Nessuna valutazione finora
- Discharge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge InstructionsDocumento3 pagineDischarge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge Instructionsacma2010Nessuna valutazione finora
- 2004 V 2 I 3 A 1Documento2 pagine2004 V 2 I 3 A 1acma2010Nessuna valutazione finora
- Capturing Return On Investment For Case Management Services: by Vickie Alexander Knight, RN, BS, CCMDocumento3 pagineCapturing Return On Investment For Case Management Services: by Vickie Alexander Knight, RN, BS, CCMacma2010Nessuna valutazione finora
- 2005 V 2 I 4 A 2Documento2 pagine2005 V 2 I 4 A 2acma2010Nessuna valutazione finora
- The Critical Role of Clinical Social Work in Case ManagementDocumento2 pagineThe Critical Role of Clinical Social Work in Case Managementacma2010Nessuna valutazione finora
- Black Dog Institute Online Clinic Assessment ReportDocumento7 pagineBlack Dog Institute Online Clinic Assessment ReportSna'a QiniNessuna valutazione finora
- Slave To Sensation by Nalini Singh ExtractDocumento19 pagineSlave To Sensation by Nalini Singh ExtractOrion Publishing Group100% (1)
- Jerrold Levinson-Contemplating Art-Oxford University Press Inc (2006)Documento432 pagineJerrold Levinson-Contemplating Art-Oxford University Press Inc (2006)Guillermo Jaimes BenítezNessuna valutazione finora
- Here Is The Complete List of Contract Removal Documents I Came Up With I Will Add More Here As I Come Up With The RestDocumento15 pagineHere Is The Complete List of Contract Removal Documents I Came Up With I Will Add More Here As I Come Up With The Restsnaps7850% (2)
- Session Guide For Knowledge ChannelDocumento3 pagineSession Guide For Knowledge ChannelIvan GunoNessuna valutazione finora
- Academic LanguageDocumento42 pagineAcademic LanguageJules Gajes50% (2)
- ZafolyDocumento7 pagineZafolyapi-300622282Nessuna valutazione finora
- Developing Cultural Awareness in Foreign Language Teaching PDFDocumento5 pagineDeveloping Cultural Awareness in Foreign Language Teaching PDFDulce Itzel VelazquezNessuna valutazione finora
- Unit 1 - Assignment - Defining Psych DisordersDocumento1 paginaUnit 1 - Assignment - Defining Psych Disordersapi-493788043Nessuna valutazione finora
- Sue Cowley - How To Survive Your First Year in TeachingDocumento209 pagineSue Cowley - How To Survive Your First Year in TeachingMark Fernando100% (8)
- Grade 9 HealthDocumento42 pagineGrade 9 Healthapi-141862995100% (1)
- Lesson Plan 4Documento6 pagineLesson Plan 4api-458299832Nessuna valutazione finora
- Salma Keropok LosongDocumento6 pagineSalma Keropok LosongPutera ZXeeNessuna valutazione finora
- Letter of Rec Daniel SpalingerDocumento1 paginaLetter of Rec Daniel Spalingerapi-334508830Nessuna valutazione finora
- Senior Seminar ProposalDocumento10 pagineSenior Seminar Proposalapi-445921937Nessuna valutazione finora
- God's For-BEAR-ance With Bullies-Condensed VersionDocumento205 pagineGod's For-BEAR-ance With Bullies-Condensed VersionPatricia BackoraNessuna valutazione finora
- Book Level Ii PDFDocumento11 pagineBook Level Ii PDFMaria Alvarez AmayaNessuna valutazione finora
- Research Format Grade 11Documento5 pagineResearch Format Grade 11Jasper Cayaga MorenoNessuna valutazione finora
- Stephen Edred Flowers - Contra Templum (2001)Documento12 pagineStephen Edred Flowers - Contra Templum (2001)Various Tings100% (1)
- Strategic LeadershipDocumento8 pagineStrategic LeadershipMazlina MazlanNessuna valutazione finora
- Academic Writing - Introduction (COLL)Documento21 pagineAcademic Writing - Introduction (COLL)Kainat BatoolNessuna valutazione finora
- DISSREVIEWERFINALDocumento4 pagineDISSREVIEWERFINALJohnCarlo AbogNessuna valutazione finora
- Grace Lartey Feb 2024Documento2 pagineGrace Lartey Feb 2024MelvinNessuna valutazione finora
- Translation Poject IntroductionDocumento31 pagineTranslation Poject IntroductionClaudine Marabut Tabora-RamonesNessuna valutazione finora
- Communities of Practice and Knowledge NetworksDocumento2 pagineCommunities of Practice and Knowledge Networksaprilrose gajetonNessuna valutazione finora
- XIII Virtues: An Excerpt From The Autobiography of Benjamin FranklinDocumento12 pagineXIII Virtues: An Excerpt From The Autobiography of Benjamin FranklinRuben BorromeoNessuna valutazione finora
- Social Studies v2 Ncbts-Based Let 2009 TosDocumento3 pagineSocial Studies v2 Ncbts-Based Let 2009 TosEngineerEducatorNessuna valutazione finora
- Hyperemesis GravidarumDocumento5 pagineHyperemesis GravidarumJeg B. Israel Jr.Nessuna valutazione finora
- ASYN Rodriguez PN. EssayDocumento1 paginaASYN Rodriguez PN. EssayNatalie SerranoNessuna valutazione finora
- English 10: Argumentative Thesis, Claims, and EvidenceDocumento9 pagineEnglish 10: Argumentative Thesis, Claims, and Evidencebelle cutieeNessuna valutazione finora
- If I Did It: Confessions of the KillerDa EverandIf I Did It: Confessions of the KillerValutazione: 3 su 5 stelle3/5 (133)
- Cold-Blooded: A True Story of Love, Lies, Greed, and MurderDa EverandCold-Blooded: A True Story of Love, Lies, Greed, and MurderValutazione: 4 su 5 stelle4/5 (53)
- Perfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthDa EverandPerfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthValutazione: 3.5 su 5 stelle3.5/5 (68)
- Our Little Secret: The True Story of a Teenage Killer and the Silence of a Small New England TownDa EverandOur Little Secret: The True Story of a Teenage Killer and the Silence of a Small New England TownValutazione: 4.5 su 5 stelle4.5/5 (86)
- Double Lives: True Tales of the Criminals Next DoorDa EverandDouble Lives: True Tales of the Criminals Next DoorValutazione: 4 su 5 stelle4/5 (34)
- Blood Brother: 33 Reasons My Brother Scott Peterson Is GuiltyDa EverandBlood Brother: 33 Reasons My Brother Scott Peterson Is GuiltyValutazione: 3 su 5 stelle3/5 (57)
- Altamont: The Rolling Stones, the Hells Angels, and the Inside Story of Rock's Darkest DayDa EverandAltamont: The Rolling Stones, the Hells Angels, and the Inside Story of Rock's Darkest DayValutazione: 4 su 5 stelle4/5 (25)
- To the Bridge: A True Story of Motherhood and MurderDa EverandTo the Bridge: A True Story of Motherhood and MurderValutazione: 4 su 5 stelle4/5 (73)
- Little Shoes: The Sensational Depression-Era Murders That Became My Family's SecretDa EverandLittle Shoes: The Sensational Depression-Era Murders That Became My Family's SecretValutazione: 4 su 5 stelle4/5 (75)
- Legally Dead: A Father and Son Bound by MurderDa EverandLegally Dead: A Father and Son Bound by MurderValutazione: 4.5 su 5 stelle4.5/5 (27)
- Relentless Pursuit: A True Story of Family, Murder, and the Prosecutor Who Wouldn't QuitDa EverandRelentless Pursuit: A True Story of Family, Murder, and the Prosecutor Who Wouldn't QuitValutazione: 4.5 su 5 stelle4.5/5 (7)
- To Kill and Kill Again: The Terrifying True Story of Montana's Baby-Faced Serial Sex MurdererDa EverandTo Kill and Kill Again: The Terrifying True Story of Montana's Baby-Faced Serial Sex MurdererValutazione: 4.5 su 5 stelle4.5/5 (157)
- Ordinary Men: Reserve Police Battalion 101 and the Final Solution in PolandDa EverandOrdinary Men: Reserve Police Battalion 101 and the Final Solution in PolandValutazione: 4.5 su 5 stelle4.5/5 (121)
- Duped: Why Innocent People Confess – and Why We Believe Their ConfessionsDa EverandDuped: Why Innocent People Confess – and Why We Believe Their ConfessionsValutazione: 4.5 su 5 stelle4.5/5 (8)
- Kilo: Inside the Deadliest Cocaine Cartels—From the Jungles to the StreetsDa EverandKilo: Inside the Deadliest Cocaine Cartels—From the Jungles to the StreetsValutazione: 4.5 su 5 stelle4.5/5 (2)
- The Poison Tree: A True Story of Family TerrorDa EverandThe Poison Tree: A True Story of Family TerrorValutazione: 4 su 5 stelle4/5 (62)
- A Deadly Game: The Untold Story of the Scott Peterson InvestigationDa EverandA Deadly Game: The Untold Story of the Scott Peterson InvestigationValutazione: 4 su 5 stelle4/5 (48)
- The Grim Sleeper: The Lost Women of South CentralDa EverandThe Grim Sleeper: The Lost Women of South CentralValutazione: 4.5 su 5 stelle4.5/5 (78)
- The True Believer: Thoughts on the Nature of Mass MovementsDa EverandThe True Believer: Thoughts on the Nature of Mass MovementsValutazione: 3.5 su 5 stelle3.5/5 (3)
- The Furies: Women, Vengeance, and JusticeDa EverandThe Furies: Women, Vengeance, and JusticeValutazione: 4.5 su 5 stelle4.5/5 (3)
- Cary Stayner: The True Story of The Yosemite Park KillerDa EverandCary Stayner: The True Story of The Yosemite Park KillerValutazione: 4 su 5 stelle4/5 (28)
- The Better Angels of Our Nature: Why Violence Has DeclinedDa EverandThe Better Angels of Our Nature: Why Violence Has DeclinedValutazione: 4 su 5 stelle4/5 (414)
- Correction: Parole, Prison, and the Possibility of ChangeDa EverandCorrection: Parole, Prison, and the Possibility of ChangeValutazione: 5 su 5 stelle5/5 (2)
- The Anatomy of Motive: The FBI's Legendary Mindhunter Explores the Key to Understanding and Catching Violent CriminalsDa EverandThe Anatomy of Motive: The FBI's Legendary Mindhunter Explores the Key to Understanding and Catching Violent CriminalsValutazione: 4 su 5 stelle4/5 (217)
- Cobalt Red: How the Blood of the Congo Powers Our LivesDa EverandCobalt Red: How the Blood of the Congo Powers Our LivesValutazione: 5 su 5 stelle5/5 (59)