Potrebbero piacerti anche
- Peads NotesDocumento18 paginePeads Notesechofox11Nessuna valutazione finora
- JaundiceDocumento53 pagineJaundiceAbhishiktaAbhiNessuna valutazione finora
- Bates Outline of Chapter 8Documento15 pagineBates Outline of Chapter 8KatherynSotoNessuna valutazione finora
- Abdominal Cavity, Peritoneum, Abdominal EsophagusDocumento4 pagineAbdominal Cavity, Peritoneum, Abdominal EsophagusMlcnd TanNessuna valutazione finora
- X Ray SchemeDocumento6 pagineX Ray SchemeIdiAmadouNessuna valutazione finora
- NEPHROTIC SYNDROME - HamidDocumento20 pagineNEPHROTIC SYNDROME - HamidAbdul Hamid OmarNessuna valutazione finora
- Doctors Charges-Thirteenth ScheduleDocumento60 pagineDoctors Charges-Thirteenth ScheduleMohd Syariefudien Mohd AriffinNessuna valutazione finora
- ENT 1.2 Diseases of The Nose, Paranasal Sinuses, and Face PDFDocumento18 pagineENT 1.2 Diseases of The Nose, Paranasal Sinuses, and Face PDFZazaNessuna valutazione finora
- Pneumothorax & Hemothorax: Farshid MokhberiDocumento32 paginePneumothorax & Hemothorax: Farshid MokhberiYan Sheng HoNessuna valutazione finora
- History Taking ExaminationDocumento7 pagineHistory Taking ExaminationIndunil AnuruddhikaNessuna valutazione finora
- Afrisya Bimo Siwendro Marisha Yadian Putri Preceptor: DR - Liza Nursanty, Spb. FinacsDocumento32 pagineAfrisya Bimo Siwendro Marisha Yadian Putri Preceptor: DR - Liza Nursanty, Spb. FinacsirmaNessuna valutazione finora
- Acute Poststreptococcal GlomerulonephritisDocumento69 pagineAcute Poststreptococcal GlomerulonephritisJirran CabatinganNessuna valutazione finora
- Disorders of Motility2Documento46 pagineDisorders of Motility2valdomiroNessuna valutazione finora
- Pleural EffusionsDocumento79 paginePleural EffusionsDiana_anca6Nessuna valutazione finora
- HerniaDocumento16 pagineHerniaVetrivel TamizhNessuna valutazione finora
- Anatomy of Thyroid GlandDocumento12 pagineAnatomy of Thyroid GlandBinbinbabu BinuNessuna valutazione finora
- Approach To Pleura LeffusionDocumento91 pagineApproach To Pleura Leffusionrodie1050% (1)
- Shouldice Paper FinalDocumento27 pagineShouldice Paper Finalclemk007Nessuna valutazione finora
- Congenital Heart DiseaseDocumento45 pagineCongenital Heart DiseaseBrandedlovers OnlineshopNessuna valutazione finora
- Approach To Cough and HemoptysisDocumento24 pagineApproach To Cough and Hemoptysisbansaleliza26Nessuna valutazione finora
- Community-Acquired Pneumonia - CPG 2016Documento26 pagineCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNessuna valutazione finora
- Gastrointestinal Tract PathologyDocumento12 pagineGastrointestinal Tract PathologyTurinawe Bin ByensiNessuna valutazione finora
- Active Listening HANDOUT PDFDocumento26 pagineActive Listening HANDOUT PDFMiguel Cuevas DolotNessuna valutazione finora
- BcqsDocumento38 pagineBcqsAdnan MaroofNessuna valutazione finora
- Chest Trauma3Documento120 pagineChest Trauma3Rojelle LezamaNessuna valutazione finora
- Anatomy - Anterior Triangle of The Neck PDFDocumento6 pagineAnatomy - Anterior Triangle of The Neck PDFAngel KimNessuna valutazione finora
- Inguinal Hernia by Dr. TalabiDocumento16 pagineInguinal Hernia by Dr. TalabidayomanNessuna valutazione finora
- PATHODocumento3 paginePATHODr-Irfan Habib100% (1)
- Mcqs Mock Exams For General Surgery Board ExamDocumento7 pagineMcqs Mock Exams For General Surgery Board ExamSergiu CiobanuNessuna valutazione finora
- Surgery Signs, Triads N SyndromesDocumento11 pagineSurgery Signs, Triads N Syndromesdrusmansaleem100% (1)
- 2022 2023 Hesi Pediatric Peds Exit Actual Exam Version 1 and 2 v1 v2 All Q As Brand NewDocumento33 pagine2022 2023 Hesi Pediatric Peds Exit Actual Exam Version 1 and 2 v1 v2 All Q As Brand NewCecilia100% (1)
- Renal PathDocumento71 pagineRenal PathSuha AbdullahNessuna valutazione finora
- PerineumDocumento4 paginePerineumwiwin09Nessuna valutazione finora
- Effectiveness of Transdermal MagnesiumDocumento2 pagineEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- Allergic Fungal Sinusitis PresentationDocumento50 pagineAllergic Fungal Sinusitis PresentationdrdrsuryaprakashNessuna valutazione finora
- Stoma Siting - Iful Syarif Al MunawiDocumento17 pagineStoma Siting - Iful Syarif Al MunawiRamdhani MaulanaNessuna valutazione finora
- #9 Ie 8 PDFDocumento8 pagine#9 Ie 8 PDFOmar BasimNessuna valutazione finora
- Thyroid Examination and ThyroidectomyDocumento9 pagineThyroid Examination and ThyroidectomyAhmadNessuna valutazione finora
- Anesthesia Pocket Cards 7 18 18Documento6 pagineAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNessuna valutazione finora
- Inguinal HerniaDocumento7 pagineInguinal HerniaNader Smadi60% (5)
- Diseases of Blood Vessels Dr. Fe A. Bartolome, Maed, FpasmapDocumento15 pagineDiseases of Blood Vessels Dr. Fe A. Bartolome, Maed, FpasmapJayesh MahajanNessuna valutazione finora
- Rhino SinusitisDocumento57 pagineRhino SinusitisArif MohammedNessuna valutazione finora
- Respiratory System Pathology (Part 1)Documento8 pagineRespiratory System Pathology (Part 1)chrisp7Nessuna valutazione finora
- Image Interpretation 4Documento93 pagineImage Interpretation 4NanaJaeNessuna valutazione finora
- PathologyDocumento28 paginePathologyninja-2001Nessuna valutazione finora
- Antiemetic Prophylaxis For CINV NEJM 2016Documento12 pagineAntiemetic Prophylaxis For CINV NEJM 2016tcd_usaNessuna valutazione finora
- Pancreatic Cancer: Pathophysiologic EtiologyDocumento2 paginePancreatic Cancer: Pathophysiologic EtiologyCharissa Magistrado De LeonNessuna valutazione finora
- EAR MCQs Points Rida NaqviDocumento6 pagineEAR MCQs Points Rida NaqviÅli Raza ChaudaryNessuna valutazione finora
- Pathology of Digestive SystemDocumento28 paginePathology of Digestive SystemDianNursyifaRahmahNessuna valutazione finora
- 149 First Aid CH 06 General Pathology FlashcardsDocumento23 pagine149 First Aid CH 06 General Pathology FlashcardsSomiZafarNessuna valutazione finora
- Study Notes Respiratory SystemDocumento19 pagineStudy Notes Respiratory SystemAnde Mangkuluhur Azhari ThalibbanNessuna valutazione finora
- Lung AbcessDocumento12 pagineLung AbcessABI OFFICIALNessuna valutazione finora
- BCQsDocumento9 pagineBCQsFarrukh Ali Khan0% (1)
- Abdominal Trauma: Fatin Amirah KamaruddinDocumento29 pagineAbdominal Trauma: Fatin Amirah Kamaruddinvirz23Nessuna valutazione finora
- Xray AbdominalDocumento38 pagineXray Abdominalrizki sanNessuna valutazione finora
- Pleural DiseasesDocumento4 paginePleural DiseasesJennifer DayNessuna valutazione finora
- Lecture 7 ThermoregulationDocumento30 pagineLecture 7 ThermoregulationLouella Artates100% (1)
- Atherosclerosis 1Documento45 pagineAtherosclerosis 1MoonAIRNessuna valutazione finora
- The Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocumento19 pagineThe Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PAAnonymous D29e00Nessuna valutazione finora
- Cranial Fossa Notes - HelpfulDocumento4 pagineCranial Fossa Notes - HelpfulKo HakuNessuna valutazione finora
- Ent SignsDocumento10 pagineEnt SignsPrasun Sit SharmaNessuna valutazione finora
- 3 Renal Vascular Disease 3Documento46 pagine3 Renal Vascular Disease 3Coy NuñezNessuna valutazione finora
- ENDOCRINE PATHOLOGY WebpathDocumento35 pagineENDOCRINE PATHOLOGY Webpathapi-3766657Nessuna valutazione finora
- #Disease of External EarDocumento4 pagine#Disease of External EarameerabestNessuna valutazione finora
- Fcps Past Papers ExamplesDocumento93 pagineFcps Past Papers ExamplesBilal Muhammad100% (1)
- Git PathologyDocumento113 pagineGit PathologyanggitaNessuna valutazione finora
- Examining The PrecordiumDocumento83 pagineExamining The PrecordiumnicolNessuna valutazione finora
- 3 Surgery - Mediastinum and PleuraDocumento6 pagine3 Surgery - Mediastinum and PleuraCassey Koi FarmNessuna valutazione finora
- Peptic Ulcers: DR Yotham Phiri Mmed (Surg)Documento46 paginePeptic Ulcers: DR Yotham Phiri Mmed (Surg)Emmanuel MukukaNessuna valutazione finora
- Pathology of The Lung: Djumadi AchmadDocumento26 paginePathology of The Lung: Djumadi AchmadVivi DeviyanaNessuna valutazione finora
- PSB 368Documento6 paginePSB 368Miguel Cuevas DolotNessuna valutazione finora
- Covid 19 CPR 7 RulesDocumento21 pagineCovid 19 CPR 7 RulesMiguel Cuevas DolotNessuna valutazione finora
- Covid 19 CPR 7 RulesDocumento21 pagineCovid 19 CPR 7 RulesMiguel Cuevas DolotNessuna valutazione finora
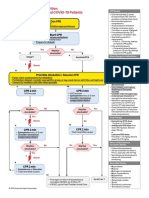
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDocumento1 paginaACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoNessuna valutazione finora
- (MED) COVID-19 Trans V. 2.0Documento6 pagine(MED) COVID-19 Trans V. 2.0Isabel VinasNessuna valutazione finora
- How Can Patients Visitors Help - May18Documento2 pagineHow Can Patients Visitors Help - May18Miguel Cuevas DolotNessuna valutazione finora
- Pedia Tickler Update 2017Documento2 paginePedia Tickler Update 2017Tani BokNessuna valutazione finora
- Clinical AbstractDocumento4 pagineClinical AbstractMiguel Cuevas DolotNessuna valutazione finora
- Physical Examination in ENT: Ussana Promyothin, MDDocumento60 paginePhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNessuna valutazione finora
- Physical Examination in ENT: Ussana Promyothin, MDDocumento60 paginePhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNessuna valutazione finora
- Vertigo Gail Ishiyama 1 13 10Documento40 pagineVertigo Gail Ishiyama 1 13 10Myname Rama LienNessuna valutazione finora
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Documento30 pagineClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNessuna valutazione finora
- Covid 19 PDFDocumento18 pagineCovid 19 PDFMiguel Cuevas DolotNessuna valutazione finora
- Physical Assessment: Ear, Nose, Mouth, and ThroatDocumento59 paginePhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNessuna valutazione finora
- Benign Paroxysmal Positional Vertigo: Waseem WatadDocumento37 pagineBenign Paroxysmal Positional Vertigo: Waseem WatadnoviNessuna valutazione finora
- Cook Book (Filipino) 13 PDFDocumento23 pagineCook Book (Filipino) 13 PDFAdina AnghelNessuna valutazione finora
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocumento12 pagineA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNessuna valutazione finora
- Neurologic ExamDocumento1 paginaNeurologic ExamMiguel Cuevas DolotNessuna valutazione finora
- Nocturnals Physiology 2018Documento14 pagineNocturnals Physiology 2018Miguel Cuevas DolotNessuna valutazione finora
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocumento12 pagineA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNessuna valutazione finora
- Drug IndexDocumento2 pagineDrug IndexMiguel Cuevas DolotNessuna valutazione finora
- Kerosene PDFDocumento31 pagineKerosene PDFRudyMLanaNessuna valutazione finora
- HEMAreviewDocumento3 pagineHEMAreviewMiguel Cuevas DolotNessuna valutazione finora
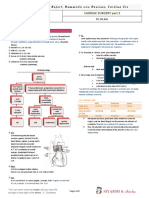
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDocumento8 pagineTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotNessuna valutazione finora
- International Journal of Surgery: Nikolaos S. Salemis, Stavros Gourgiotis, Georgios KaralisDocumento4 pagineInternational Journal of Surgery: Nikolaos S. Salemis, Stavros Gourgiotis, Georgios KaralisKinandanaNessuna valutazione finora
- Hernia: A General Term Referring To A Protrusion of A: TissueDocumento3 pagineHernia: A General Term Referring To A Protrusion of A: TissueVictor ElvisNessuna valutazione finora
- Combined Okell NotesDocumento202 pagineCombined Okell Notessameeramw100% (5)
- Css CT Scan AbdomenDocumento54 pagineCss CT Scan AbdomenUlfa DiyaNessuna valutazione finora
- Open Inguinal Hernia Repair Lichtenstein CadaverDocumento9 pagineOpen Inguinal Hernia Repair Lichtenstein CadaverTeja Laksana NukanaNessuna valutazione finora
- Anaesthesia For A Rare Case of Down's Syndrome With Morgagni's Hernia Undergoing Laparoscopic RepairDocumento2 pagineAnaesthesia For A Rare Case of Down's Syndrome With Morgagni's Hernia Undergoing Laparoscopic Repairnethra nitinNessuna valutazione finora
- Symptomatic Bochdalek Hernia in An AdultDocumento4 pagineSymptomatic Bochdalek Hernia in An Adultika nur utamiNessuna valutazione finora
- Case Taking Proforma in ABDOMINAL LUMPDocumento4 pagineCase Taking Proforma in ABDOMINAL LUMPSrishtiNessuna valutazione finora
- Physiqz Sports Hernia Master Guide 1Documento65 paginePhysiqz Sports Hernia Master Guide 1Pablo CuriaNessuna valutazione finora
- Modul Digestive Blok 9Documento25 pagineModul Digestive Blok 9prabuNessuna valutazione finora
- List of General SurgeriesDocumento9 pagineList of General SurgeriesNarayanan RajendranNessuna valutazione finora
- TAPP HernioplastyDocumento5 pagineTAPP HernioplastyMaryam Alam KhanNessuna valutazione finora
- Baumann 2018Documento13 pagineBaumann 2018Sisca Dwi AgustinaNessuna valutazione finora
- CGHS Rate GuwahatiDocumento54 pagineCGHS Rate GuwahatiJeremy Remlalfaka100% (4)
- HidroceleDocumento4 pagineHidroceleAnshy V. FreireNessuna valutazione finora
- HerniaDocumento21 pagineHerniaMunungwe WìllíâmNessuna valutazione finora
- Surgery Series Part 1 Lichtenstein's Hernioplasty PDFDocumento23 pagineSurgery Series Part 1 Lichtenstein's Hernioplasty PDFC.Naveen AntonyNessuna valutazione finora
- Git Surgery 4 Year 2022 NebrasDocumento9 pagineGit Surgery 4 Year 2022 NebrasHazemAbu-BakrNessuna valutazione finora
- Surgery II - Topical Past Papers (2007-2019)Documento61 pagineSurgery II - Topical Past Papers (2007-2019)AnmahNessuna valutazione finora
- A 27-Year-Old Woman Presented With Three-Day History of Generalized Mild Abdominal PainDocumento144 pagineA 27-Year-Old Woman Presented With Three-Day History of Generalized Mild Abdominal PainAldredNessuna valutazione finora
- Pediatric Surgery Departement Statistics Alexandria EgyptDocumento30 paginePediatric Surgery Departement Statistics Alexandria Egypthayssam rashwanNessuna valutazione finora
- Diagnostic Laparoscopy: Consent Advice No. 2Documento8 pagineDiagnostic Laparoscopy: Consent Advice No. 2Sapna SNessuna valutazione finora
- CME Trunk, Abdomen, and Pressure Sore ReconstructionDocumento15 pagineCME Trunk, Abdomen, and Pressure Sore ReconstructionVeronica TomaselloNessuna valutazione finora