Potrebbero piacerti anche
- Approach To Diagnosis of Haemolytic AnaemiasDocumento2 pagineApproach To Diagnosis of Haemolytic AnaemiasGerardLumNessuna valutazione finora
- Bone Marrow FailureDocumento2 pagineBone Marrow FailureGerardLum100% (1)
- Overview of AnaemiaDocumento2 pagineOverview of AnaemiaGerardLumNessuna valutazione finora
- Leukocytes Benign DisordersDocumento3 pagineLeukocytes Benign DisordersGerardLum100% (3)
- Female Genital TractDocumento5 pagineFemale Genital Tractsarguss14100% (1)
- IM NotesDocumento79 pagineIM NotesInri Dumlao100% (1)
- Pathology of TestesDocumento4 paginePathology of TestesGerardLum100% (1)
- Acute Lymphoblastic Leukemia QuestionsDocumento22 pagineAcute Lymphoblastic Leukemia Questionsđoàn lươngNessuna valutazione finora
- Hematologic Pathology p36-47Documento12 pagineHematologic Pathology p36-47zeroun24Nessuna valutazione finora
- Hem-Onc: AnswerDocumento3 pagineHem-Onc: AnswerAman Raj KNessuna valutazione finora
- Breast CancerDocumento6 pagineBreast Cancersarguss14Nessuna valutazione finora
- IM Part 1 and 2 CombinedDocumento100 pagineIM Part 1 and 2 CombinedsasghfdgNessuna valutazione finora
- The Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract InfectionsDocumento4 pagineThe Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract Infectionssarguss14Nessuna valutazione finora
- Peptic UlcerDocumento4 paginePeptic UlcerEris Abdul AzizNessuna valutazione finora
- Introduction To TransplantationDocumento3 pagineIntroduction To TransplantationGerardLumNessuna valutazione finora
- Hodgkins and Non Hodgkins LymphomaDocumento5 pagineHodgkins and Non Hodgkins LymphomakakuNessuna valutazione finora
- WBC Neoplasms Review - PathologyDocumento6 pagineWBC Neoplasms Review - Pathologylas100% (6)
- Leukemias & Lymphomas - HY USMLEDocumento87 pagineLeukemias & Lymphomas - HY USMLEMatt McGlothlinNessuna valutazione finora
- Female PathologyDocumento16 pagineFemale Pathologymiguel cuevasNessuna valutazione finora
- (MED II) 1.05 Emergencies in Cancer PatientsDocumento17 pagine(MED II) 1.05 Emergencies in Cancer PatientsJearwin AngelesNessuna valutazione finora
- Tumour Marker For Medincine ResidentsDocumento58 pagineTumour Marker For Medincine ResidentsSandeep NarayananNessuna valutazione finora
- Diseases of The Female Genital TractDocumento4 pagineDiseases of The Female Genital Tractsarguss14Nessuna valutazione finora
- Decreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisDocumento8 pagineDecreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisSamuel RothschildNessuna valutazione finora
- Mohammad Altamimi, MD, PHD Jordan UniversityDocumento16 pagineMohammad Altamimi, MD, PHD Jordan UniversityDaniel AtiehNessuna valutazione finora
- Pathology Week 5 p1-14Documento20 paginePathology Week 5 p1-14zeroun24100% (1)
- Acquired Bleeding DisordersDocumento1 paginaAcquired Bleeding DisordersGerardLumNessuna valutazione finora
- CH 7 Genetic and Pediatric Diseases (P. 243-272, Nature of Genetic Abnormalities Contributing To Human DiseaseDocumento16 pagineCH 7 Genetic and Pediatric Diseases (P. 243-272, Nature of Genetic Abnormalities Contributing To Human DiseaseJustine HungNessuna valutazione finora
- Pathology GlomerulonephritisDocumento4 paginePathology GlomerulonephritisGerardLum100% (2)
- ENDOCRINE PATHOLOGY WebpathDocumento35 pagineENDOCRINE PATHOLOGY Webpathapi-3766657Nessuna valutazione finora
- Acute Post Streptococcal Glomerulonephritis: DiseaseDocumento3 pagineAcute Post Streptococcal Glomerulonephritis: DiseaseHades Luciferos PallonesNessuna valutazione finora
- IKD9 - Radiological Evaluation of Renal CystsDocumento26 pagineIKD9 - Radiological Evaluation of Renal CystsRenal Association MauritiusNessuna valutazione finora
- 02 Clin Path-WBC Disorders PDFDocumento12 pagine02 Clin Path-WBC Disorders PDFRobert Dominic GonzalesNessuna valutazione finora
- Laboratorial Diagnostics Keypoints RevisionDocumento6 pagineLaboratorial Diagnostics Keypoints RevisionFathimathNessuna valutazione finora
- Surgical Anatomy of The Chest Wall, Pleura, and MediastinumDocumento8 pagineSurgical Anatomy of The Chest Wall, Pleura, and MediastinumNooneNessuna valutazione finora
- (MICROA - 2.1) Myeloid Tissue HistologyDocumento6 pagine(MICROA - 2.1) Myeloid Tissue HistologyHenryboi CañasNessuna valutazione finora
- Pathology of Female Genital Tract Short NotesDocumento5 paginePathology of Female Genital Tract Short NotesameerabestNessuna valutazione finora
- FMS 1 - Week 7 Tutorial 1 LO PDFDocumento17 pagineFMS 1 - Week 7 Tutorial 1 LO PDFAprillia AlmaasNessuna valutazione finora
- Abnormal CBC - PresentationDocumento23 pagineAbnormal CBC - PresentationMateen ShukriNessuna valutazione finora
- Chronic Myeloid LeukaemiaDocumento44 pagineChronic Myeloid Leukaemiaapi-273068056Nessuna valutazione finora
- Benign Gynecologic Lesions FinalDocumento11 pagineBenign Gynecologic Lesions Final2012100% (4)
- Hematologic Pathology p65-87Documento23 pagineHematologic Pathology p65-87zeroun24100% (1)
- Clinical CasesDocumento86 pagineClinical Caseshanyedward5005446Nessuna valutazione finora
- Hafizuddin Mohamed Fauzi P-UM0037/10Documento54 pagineHafizuddin Mohamed Fauzi P-UM0037/10Hafizuddin Mohamed FauziNessuna valutazione finora
- Midterm Chapter7Documento43 pagineMidterm Chapter7Frances FranciscoNessuna valutazione finora
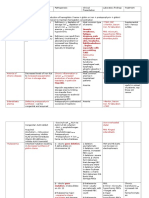
- Disease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesDocumento11 pagineDisease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesSara AshurstNessuna valutazione finora
- Pathology Week 6 p18-35Documento18 paginePathology Week 6 p18-35zeroun24Nessuna valutazione finora
- Myelodysplastic Syndromes Hematology 1: 1. MDS With Multilineage Dysplasia (MDS-MLD)Documento9 pagineMyelodysplastic Syndromes Hematology 1: 1. MDS With Multilineage Dysplasia (MDS-MLD)Joezer Gumangan VeranoNessuna valutazione finora
- A Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Thyroid PhysiologyDocumento2 pagineThyroid PhysiologyGerardLum100% (2)
- Clinical Medicine - Lecture: - Topic: - DateDocumento3 pagineClinical Medicine - Lecture: - Topic: - DateqselmmNessuna valutazione finora
- Hematologic Pathology p1-23Documento23 pagineHematologic Pathology p1-23zeroun24100% (2)
- HaematinicsDocumento2 pagineHaematinicsGerardLum100% (2)
- Rheumatic Fever and Rheumatic Heart DiseaseDocumento132 pagineRheumatic Fever and Rheumatic Heart DiseaseDamie FernandezNessuna valutazione finora
- RBC MorphologyDocumento9 pagineRBC MorphologybiancsNessuna valutazione finora
- Myeloproliferative DisordersDocumento2 pagineMyeloproliferative DisordersGerardLumNessuna valutazione finora
- Lymphoma (Ean's) - 2Documento29 pagineLymphoma (Ean's) - 2eanfital11Nessuna valutazione finora
- Fast Facts: Myelodysplastic Syndromes: Determining risk, tailoring therapy, supporting patientsDa EverandFast Facts: Myelodysplastic Syndromes: Determining risk, tailoring therapy, supporting patientsNessuna valutazione finora
- ThalassaemiaDocumento4 pagineThalassaemiaGerardLum100% (4)
- Vesico Ureteral RefluxDocumento1 paginaVesico Ureteral RefluxGerardLumNessuna valutazione finora
- Thyroid PhysiologyDocumento2 pagineThyroid PhysiologyGerardLum100% (2)
- Urinary Tract InfectionDocumento4 pagineUrinary Tract InfectionGerardLum100% (2)
- ThrombophiliaDocumento3 pagineThrombophiliaGerardLum100% (1)
- Urinary Tract Infections in ChildrenDocumento1 paginaUrinary Tract Infections in ChildrenGerardLumNessuna valutazione finora
- Prostate GlandsDocumento3 pagineProstate GlandsDragan PetrovicNessuna valutazione finora
- Skeletal Muscle RelaxantsDocumento1 paginaSkeletal Muscle RelaxantsGerardLum100% (2)
- Soft Tissue TumoursDocumento8 pagineSoft Tissue TumoursGerardLum100% (2)
- Renal Function in Disease StateDocumento2 pagineRenal Function in Disease Statedamai140390Nessuna valutazione finora
- Sexually Transmitted DiseasesDocumento6 pagineSexually Transmitted DiseasesGerardLum100% (3)
- Pathogenesis Bleeding DisordersDocumento4 paginePathogenesis Bleeding DisordersGerardLumNessuna valutazione finora
- Soft Tissue InfectionsDocumento3 pagineSoft Tissue InfectionsGerardLum100% (1)
- Renal Excretion of DrugsDocumento3 pagineRenal Excretion of DrugsGerardLum100% (3)
- Pathology of TestesDocumento4 paginePathology of TestesGerardLum100% (1)
- Posterior Pituitary SyndromeDocumento1 paginaPosterior Pituitary SyndromeGerardLumNessuna valutazione finora
- Principles of Blood TransfusionDocumento2 paginePrinciples of Blood TransfusionGerardLum100% (3)
- Pathophysiology of Calcium, Phosphate HomeostasisDocumento5 paginePathophysiology of Calcium, Phosphate HomeostasisGerardLum100% (1)
- Pathophysiology of Nerve InjuryDocumento2 paginePathophysiology of Nerve InjuryGerardLum100% (1)
- Pituitary DysfunctionDocumento2 paginePituitary DysfunctionGerardLum0% (1)
- Pathology of DiabetesDocumento4 paginePathology of DiabetesGerardLum100% (4)
- Pathology GlomerulonephritisDocumento4 paginePathology GlomerulonephritisGerardLum100% (2)
- Pathogenesis Chronic Complications DiabetesDocumento5 paginePathogenesis Chronic Complications DiabetesGerardLum100% (1)
- Pituitary Gland PathologyDocumento4 paginePituitary Gland PathologyGerardLumNessuna valutazione finora
- Pathology of Thyroid DiseasesDocumento5 paginePathology of Thyroid DiseasesGerardLum100% (2)
- Paediatrics OrthopaedicsDocumento5 paginePaediatrics OrthopaedicsGerardLumNessuna valutazione finora
- Nocturnal EnuresisDocumento1 paginaNocturnal EnuresisGerardLumNessuna valutazione finora
- Obstructive UropathyDocumento3 pagineObstructive UropathyGerardLum100% (1)
- Nsaids DrugsDocumento2 pagineNsaids DrugsIrene Zae MwandotoNessuna valutazione finora
- 4 Ophthalmologists Cullman, AL: We Found NearDocumento2 pagine4 Ophthalmologists Cullman, AL: We Found NearSantosh Sharma VaranasiNessuna valutazione finora
- Four Big Pollution Diseases of Japan - Wikipedia, The Free Encyclopedia PDFDocumento6 pagineFour Big Pollution Diseases of Japan - Wikipedia, The Free Encyclopedia PDFudayngNessuna valutazione finora
- NCP Case PresDocumento5 pagineNCP Case Pressyd19Nessuna valutazione finora
- Krok 2 2002-2003 SurgeryDocumento23 pagineKrok 2 2002-2003 SurgeryAli ZeeshanNessuna valutazione finora
- The Following Resources Related To This Article Are Available Online atDocumento8 pagineThe Following Resources Related To This Article Are Available Online atFerdina NidyasariNessuna valutazione finora
- Immune Response To Infectious DiseaseDocumento2 pagineImmune Response To Infectious Diseasekiedd_04100% (1)
- Danish Mask StudyDocumento1 paginaDanish Mask StudyJuana AtkinsNessuna valutazione finora
- Online Review Exam ISBBDocumento44 pagineOnline Review Exam ISBBRockét PeredoNessuna valutazione finora
- Efficacy of Glimepiride/metformin Combination Versus Glibenclamide/ Metformin in Patients With Uncontrolled Type 2 Diabetes MellitusDocumento4 pagineEfficacy of Glimepiride/metformin Combination Versus Glibenclamide/ Metformin in Patients With Uncontrolled Type 2 Diabetes Mellitusfannia nabillaNessuna valutazione finora
- Lung Adenocarcinoma Case PresentationDocumento29 pagineLung Adenocarcinoma Case PresentationthekidthatcantNessuna valutazione finora
- Kizilarslanoglu 2016Documento7 pagineKizilarslanoglu 2016EviNessuna valutazione finora
- Nonoperative Management of Femoroacetabular ImpingementDocumento8 pagineNonoperative Management of Femoroacetabular ImpingementRodrigo SantosNessuna valutazione finora
- Occupational Safety and HealthDocumento9 pagineOccupational Safety and HealthWan SaitamaNessuna valutazione finora
- BLS Aha - 2010 Refresher Course For Junior Clerks 2015Documento28 pagineBLS Aha - 2010 Refresher Course For Junior Clerks 2015Kalpana ShahNessuna valutazione finora
- Massage Therapy - Basic Techniques of Swedish Massage - Massage - Therapeutic Massage - Swedish MassageDocumento1 paginaMassage Therapy - Basic Techniques of Swedish Massage - Massage - Therapeutic Massage - Swedish MassagenaveenNessuna valutazione finora
- Priyanka Sen Final Practice School Internship ReportDocumento35 paginePriyanka Sen Final Practice School Internship ReportThakur Aditya PratapNessuna valutazione finora
- Nursing DiagnosisDocumento3 pagineNursing DiagnosislesternNessuna valutazione finora
- Sudeep SrivastavaDocumento202 pagineSudeep Srivastavasandeepsrivastava41Nessuna valutazione finora
- Actinic KeratosisDocumento19 pagineActinic KeratosisDajour CollinsNessuna valutazione finora
- Chapter 21 - Nursing Care of The Family During The Postpartum PeriodDocumento11 pagineChapter 21 - Nursing Care of The Family During The Postpartum PeriodJill Hill100% (3)
- Maternal Care and ServicesDocumento35 pagineMaternal Care and ServicesAaron ConstantinoNessuna valutazione finora
- Dosis Antibiotik: November 2015Documento8 pagineDosis Antibiotik: November 2015subchaan waruNessuna valutazione finora
- Nicaragua Reflection PaperDocumento3 pagineNicaragua Reflection Paperapi-487254609Nessuna valutazione finora
- NEET-SS UrologyDocumento59 pagineNEET-SS Urologyadi100% (1)
- Test Bank For Health Psychology 7th Edition TaylorDocumento21 pagineTest Bank For Health Psychology 7th Edition Taylorwoodwardpunction2vq46zNessuna valutazione finora
- Status Asthmaticus Case StudyDocumento18 pagineStatus Asthmaticus Case Studygeorgeloto12Nessuna valutazione finora
- CraniomaDocumento7 pagineCraniomaSophia BeecherNessuna valutazione finora
- West African Journal of Medicine: Volume 40, Number 1 January 2023Documento12 pagineWest African Journal of Medicine: Volume 40, Number 1 January 2023ThankGod OgbonnaNessuna valutazione finora
- IMA Monthly Report Form JulyDocumento4 pagineIMA Monthly Report Form JulyInternetStudioNessuna valutazione finora
- LINKSERVE Training MaterialsDocumento15 pagineLINKSERVE Training MaterialslisingynnamaeNessuna valutazione finora