Potrebbero piacerti anche
- Lenalidomide Plus Rituximab As Initial Treatment For Mantle-Cell LymphomaDocumento10 pagineLenalidomide Plus Rituximab As Initial Treatment For Mantle-Cell LymphomaSECOELUNICONessuna valutazione finora
- Minimal Morphological Criteria For Defining Bone MarrowDocumento10 pagineMinimal Morphological Criteria For Defining Bone MarrowSECOELUNICONessuna valutazione finora
- Refractory Anemia With Ring Sideroblasts (RARS) and RARSDocumento14 pagineRefractory Anemia With Ring Sideroblasts (RARS) and RARSSECOELUNICONessuna valutazione finora
- 4477 Full PDFDocumento14 pagine4477 Full PDFSECOELUNICONessuna valutazione finora
- Tumour Lysis Syndrome: New Therapeutic Strategies and ClassificationDocumento9 pagineTumour Lysis Syndrome: New Therapeutic Strategies and ClassificationSECOELUNICONessuna valutazione finora
- Jca TTP CC 2013Documento20 pagineJca TTP CC 2013SECOELUNICONessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Drug Study - Ello - Ampicillin - MultivitaminsDocumento3 pagineDrug Study - Ello - Ampicillin - MultivitaminsCHRISTINE GRACE ELLONessuna valutazione finora
- V1.0-Emergency Plan For Prevention and Control of New Coronavirus - Disease-CPPESEA PDFDocumento12 pagineV1.0-Emergency Plan For Prevention and Control of New Coronavirus - Disease-CPPESEA PDFNutthakarn WisatsiriNessuna valutazione finora
- Vaginal Prolapse: by DR MutevheDocumento32 pagineVaginal Prolapse: by DR MutevhedanielNessuna valutazione finora
- Tetanus: Guerrero, Djameica Danielle RDocumento16 pagineTetanus: Guerrero, Djameica Danielle RDjameica GuerreroNessuna valutazione finora
- Garssen, 2004 - Physical Training and Fatigue, Fitness, and Quality of Life in Guillain-Barre Syndrome and CIDPDocumento3 pagineGarssen, 2004 - Physical Training and Fatigue, Fitness, and Quality of Life in Guillain-Barre Syndrome and CIDPkarinaNessuna valutazione finora
- AZ Heart Angioscreen - Biltmore Lifestyles Dec 2022Documento1 paginaAZ Heart Angioscreen - Biltmore Lifestyles Dec 2022Brittany LudwigNessuna valutazione finora
- What Is Heart Bypass SurgeryDocumento10 pagineWhat Is Heart Bypass SurgeryVanitha AlagarsamyNessuna valutazione finora
- Jabeen & TahirDocumento12 pagineJabeen & TahirSanaNessuna valutazione finora
- Dilated CardiomyopathyDocumento23 pagineDilated CardiomyopathyYanna Habib-MangotaraNessuna valutazione finora
- Personal Health Issues and ConcernDocumento41 paginePersonal Health Issues and Concernniña pinedaNessuna valutazione finora
- Behavior and Mental Status Can Be Early Signs of Impaired Gas ExchangeDocumento2 pagineBehavior and Mental Status Can Be Early Signs of Impaired Gas ExchangeJoanna Marie Lumbre BalbiranNessuna valutazione finora
- Hernia - Surgery PrecisDocumento1 paginaHernia - Surgery PrecisSherif WagdyNessuna valutazione finora
- Digital Covid Questionnaire For Revival Approval FormatDocumento2 pagineDigital Covid Questionnaire For Revival Approval Formatsouravdey3Nessuna valutazione finora
- Basics of Soft - Tissue ExaminationDocumento32 pagineBasics of Soft - Tissue ExaminationGurudutt PaiNessuna valutazione finora
- Pathology of Common Glomerular Syndromes: DR Purushotham KrishnappaDocumento34 paginePathology of Common Glomerular Syndromes: DR Purushotham KrishnappaTarin IslamNessuna valutazione finora
- Topical Oxygen Wound TherapyDocumento9 pagineTopical Oxygen Wound TherapyTony LeeNessuna valutazione finora
- Case 4-2021: A 70-Year-Old Woman With Dyspnea On Exertion and Abnormal Findings On Chest ImagingDocumento12 pagineCase 4-2021: A 70-Year-Old Woman With Dyspnea On Exertion and Abnormal Findings On Chest ImagingBruno ConteNessuna valutazione finora
- 114 okMSAD AFP-Differentiation and Diagnosis of Tremor PDFDocumento6 pagine114 okMSAD AFP-Differentiation and Diagnosis of Tremor PDFkasmiantoabadiNessuna valutazione finora
- Homeopathy Cases by KadwaDocumento179 pagineHomeopathy Cases by Kadwaabckadwa100% (3)
- Sexually Transmitted DiseaseDocumento38 pagineSexually Transmitted Diseaserana arslanNessuna valutazione finora
- Bhatia and Speed Grand Test McqsDocumento10 pagineBhatia and Speed Grand Test McqsRavi RajaNessuna valutazione finora
- Andaman Fever A New EntityDocumento6 pagineAndaman Fever A New EntitySheepu SharmaNessuna valutazione finora
- Slides From McCullough 10-27-2021 PresentationDocumento83 pagineSlides From McCullough 10-27-2021 PresentationAssociation of American Physicians and Surgeons100% (10)
- Hydatidiform Mole: Case Report SessionDocumento34 pagineHydatidiform Mole: Case Report SessionSelaNessuna valutazione finora
- Dr. Khairiyadi, M.Kes., Sp.A Departemen Ilmu Kesehatan Anak RSUD Ulin BanjarmasinDocumento78 pagineDr. Khairiyadi, M.Kes., Sp.A Departemen Ilmu Kesehatan Anak RSUD Ulin BanjarmasinEldhaNessuna valutazione finora
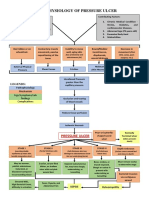
- Pathophysiology of Pressure UlcerDocumento1 paginaPathophysiology of Pressure UlcerSTORAGE FILENessuna valutazione finora
- Patho AsthmaDocumento1 paginaPatho AsthmaAyel JimenezNessuna valutazione finora
- Magic Surgery NotesDocumento54 pagineMagic Surgery NotesChimwemwe TemboNessuna valutazione finora
- C-Reactive Protein in Serum by NephelometryDocumento12 pagineC-Reactive Protein in Serum by NephelometryTrajceNessuna valutazione finora
- Epidemiological and Clinical Features of Pediatric COVID-19: Researcharticle Open AccessDocumento7 pagineEpidemiological and Clinical Features of Pediatric COVID-19: Researcharticle Open AccessAditha Fitrina AndianiNessuna valutazione finora