Potrebbero piacerti anche
- Drug ChartDocumento8 pagineDrug Chartstudentalwaysstudy100% (1)
- Microbiology Step 1 Antimicrobials ChartDocumento6 pagineMicrobiology Step 1 Antimicrobials ChartM Patel100% (1)
- Inhibitor of Cell Wall Synthesis (ICWS) : Proteus ComboDocumento12 pagineInhibitor of Cell Wall Synthesis (ICWS) : Proteus Comboflomax23100% (1)
- Antibiotics Chart 2Documento10 pagineAntibiotics Chart 2Vee MendNessuna valutazione finora
- Ninja - Anemias PDFDocumento1 paginaNinja - Anemias PDFErica Hyeyeon LeeNessuna valutazione finora
- Complete Drug GuideDocumento225 pagineComplete Drug GuideJessica 'Baker' IsaacsNessuna valutazione finora
- Antibiotics ChartDocumento10 pagineAntibiotics Chartadom09Nessuna valutazione finora
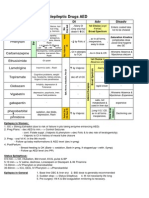
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocumento1 paginaAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Nessuna valutazione finora
- Lab Values Chart 120511 PDFDocumento5 pagineLab Values Chart 120511 PDFVanessaMUeller100% (3)
- Pharma GI CardsDocumento16 paginePharma GI CardsDoctorsHangout.comNessuna valutazione finora
- Labs Electrolyte ChartDocumento1 paginaLabs Electrolyte ChartmdcmepNessuna valutazione finora
- @ Shopwithkey On Etsy Perfusion Drug Classification ChartDocumento8 pagine@ Shopwithkey On Etsy Perfusion Drug Classification ChartSutanyaNessuna valutazione finora
- Drugclasses Pharmacologypart 1 PDFDocumento25 pagineDrugclasses Pharmacologypart 1 PDFSutanya100% (2)
- Ninja - Antihyperlipidemics PDFDocumento3 pagineNinja - Antihyperlipidemics PDFErica Hyeyeon Lee100% (1)
- Renal Guide and Charts: AlbuminDocumento16 pagineRenal Guide and Charts: AlbuminYaima JimenezNessuna valutazione finora
- Pharmacology Main DrugsDocumento14 paginePharmacology Main DrugsSabir KhanNessuna valutazione finora
- Pharmacology Chart 3Documento2 paginePharmacology Chart 3Omar ClorNessuna valutazione finora
- Soap TemplateDocumento3 pagineSoap TemplaterohitNessuna valutazione finora
- Cardiac Drugs HypertensionDocumento5 pagineCardiac Drugs HypertensionEciOwnsMeNessuna valutazione finora
- Diabetes Mellitus Drug ChartDocumento3 pagineDiabetes Mellitus Drug Chartlui.stephanie1751100% (1)
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDocumento18 paginePharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- Internal Medicine #1Documento167 pagineInternal Medicine #1Nikhil RayarakulaNessuna valutazione finora
- Lile Bai 1: Area/Site Common Organism Useful Abx Other NotesDocumento3 pagineLile Bai 1: Area/Site Common Organism Useful Abx Other NotesNicole BerryNessuna valutazione finora
- Insulin Chart 05032012 PDFDocumento1 paginaInsulin Chart 05032012 PDFTiffany CrittendenNessuna valutazione finora
- Musculoskeletal PharmacologyDocumento18 pagineMusculoskeletal PharmacologyBLEEMAGE100% (2)
- Antibacterial Drugs SummaryDocumento13 pagineAntibacterial Drugs SummaryNeo Ramagaga100% (1)
- Whole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsDocumento17 pagineWhole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsFlorina TrutescuNessuna valutazione finora
- Sphere: These DiarrheaDocumento3 pagineSphere: These Diarrheamed testNessuna valutazione finora
- Comprehensive Nclex Notes Easy To Read PDFDocumento97 pagineComprehensive Nclex Notes Easy To Read PDFKenia GeorgesNessuna valutazione finora
- Test InformationDocumento5 pagineTest InformationCatalina BorquezNessuna valutazione finora
- Med CardsDocumento4 pagineMed CardsSonia FernandesNessuna valutazione finora
- Anticoagulants Drug TableDocumento1 paginaAnticoagulants Drug Tablecdp158767% (3)
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDocumento5 paginePharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SNessuna valutazione finora
- Normal Lab ValuesDocumento3 pagineNormal Lab ValuesHNessuna valutazione finora
- Pharm TableDocumento35 paginePharm TableHannah BaldwinNessuna valutazione finora
- Pain and Inflammation Med ChartsDocumento4 paginePain and Inflammation Med Chartssurviving nursing school100% (1)
- Gastro MnemonicsDocumento8 pagineGastro MnemonicsRufina SoomroNessuna valutazione finora
- Cardiovascular Pharmacology OutlineDocumento11 pagineCardiovascular Pharmacology OutlineLhay de OcampoNessuna valutazione finora
- Template Drug Card1Documento1 paginaTemplate Drug Card1Kay TaylorNessuna valutazione finora
- Ace Inhibitors MnemonicDocumento1 paginaAce Inhibitors MnemonicGirish Waru0% (2)
- Pharmacology Notes (Chapter 20 and 21)Documento2 paginePharmacology Notes (Chapter 20 and 21)graycorypNessuna valutazione finora
- 50 Most Commonly Prescribed Medications 02Documento4 pagine50 Most Commonly Prescribed Medications 02Jelly BeanNessuna valutazione finora
- Transport of Critically Ill Adults 2011Documento1 paginaTransport of Critically Ill Adults 2011velocity25Nessuna valutazione finora
- NCLEX Review: Pharmacology Charlene Natale, BSN, RNDocumento43 pagineNCLEX Review: Pharmacology Charlene Natale, BSN, RNMenly Susada100% (1)
- AntimicrobialsDocumento1 paginaAntimicrobialsRomaine Barrett100% (1)
- GI Diarrheal Micro ChartDocumento3 pagineGI Diarrheal Micro ChartEvan MillerNessuna valutazione finora
- Cardiovascular Drugs XL ChartDocumento4 pagineCardiovascular Drugs XL Chartcdp158767% (3)
- Lippin NotesDocumento8 pagineLippin Noteswalt65100% (1)
- Nephrotic and NephriticDocumento27 pagineNephrotic and Nephritictam meiNessuna valutazione finora
- Mobic Drug CardDocumento1 paginaMobic Drug CardSheri490Nessuna valutazione finora
- Drug Interactions 2 Paper PDFDocumento2 pagineDrug Interactions 2 Paper PDFAzima AbdelrhamanNessuna valutazione finora
- Drug CardsDocumento3 pagineDrug CardsDave HillNessuna valutazione finora
- Pharmacology: Fast and Dirty Board ReviewDocumento7 paginePharmacology: Fast and Dirty Board ReviewRochelleth7278Nessuna valutazione finora
- Tuberculosis: PGI: Mikhail Jude L. OpayDocumento45 pagineTuberculosis: PGI: Mikhail Jude L. OpayMikkoOpayNessuna valutazione finora
- Drug Study CompilationDocumento9 pagineDrug Study CompilationRene John FranciscoNessuna valutazione finora
- Pharma Important Exams TopicsDocumento16 paginePharma Important Exams TopicsMd. Tanvir AhammedNessuna valutazione finora
- Anti - TB DrugsupdatedDocumento35 pagineAnti - TB DrugsupdatedgNessuna valutazione finora
- Pharmacotherapy of ENT InfectionsDocumento86 paginePharmacotherapy of ENT InfectionsHoque Mohammed Newaz ShorifulNessuna valutazione finora
- Anti Fungal DrugsDocumento6 pagineAnti Fungal Drugsbilal ahmadNessuna valutazione finora
- List of AntibioticsDocumento11 pagineList of AntibioticsD. BarNessuna valutazione finora
- Combank NotesDocumento7 pagineCombank NotesVee MendNessuna valutazione finora
- Amboss NotesDocumento12 pagineAmboss NotesVee Mend100% (2)
- Comat NotesDocumento33 pagineComat NotesVee Mend100% (1)
- UWorld Notes Step 2Documento93 pagineUWorld Notes Step 2Vee Mend100% (1)
- Comlex EthicsDocumento3 pagineComlex EthicsVee MendNessuna valutazione finora
- Session 2 Basics of NutritionDocumento39 pagineSession 2 Basics of NutritionAllyeah bethel GrupoNessuna valutazione finora
- BPH3114 - Applied Epidemiology CATDocumento2 pagineBPH3114 - Applied Epidemiology CATGideon MukalaziNessuna valutazione finora
- ASPEN Prácticas Seguras para La Nutrición EnteralDocumento89 pagineASPEN Prácticas Seguras para La Nutrición EnteralsofiaNessuna valutazione finora
- Art - Atraumatic Restorative Treatment in DentistryDocumento32 pagineArt - Atraumatic Restorative Treatment in DentistryPuneet ChoudharyNessuna valutazione finora
- Personal Development: Quarter 1 - Module 4Documento33 paginePersonal Development: Quarter 1 - Module 4JulieAnnLucasBagamaspad100% (1)
- Acute GastroenteritisDocumento63 pagineAcute GastroenteritisSathya MoorthyNessuna valutazione finora
- Differences in Mood Between Elderly Persons Living in Different Residential Environments in SloveniaDocumento9 pagineDifferences in Mood Between Elderly Persons Living in Different Residential Environments in SloveniaEstera ŽalikNessuna valutazione finora
- Formative Practice Chapter 2 (BI)Documento8 pagineFormative Practice Chapter 2 (BI)suraya nazaNessuna valutazione finora
- Impact: of Tuberculosis ON History, Literature and ArtDocumento18 pagineImpact: of Tuberculosis ON History, Literature and ArtMaria Eliza GiuboruncaNessuna valutazione finora
- Cardiovascular Diseases ListDocumento7 pagineCardiovascular Diseases ListAnant SinghNessuna valutazione finora
- Differential Diagnosis of Genital Ulcer Differential Diagnosis of Genital UlcersDocumento3 pagineDifferential Diagnosis of Genital Ulcer Differential Diagnosis of Genital UlcersNurhayati HasanahNessuna valutazione finora
- Takayasu ArteritisDocumento53 pagineTakayasu ArteritisSuruchi Jagdish Sharma50% (2)
- Definitions, Epidemiology, and Risk Factors For Inflammatory Bowel Disease - UpToDateDocumento25 pagineDefinitions, Epidemiology, and Risk Factors For Inflammatory Bowel Disease - UpToDateTurma A 2019.1 Med-FCMNessuna valutazione finora
- CoughDocumento11 pagineCoughVenkatesan VidhyaNessuna valutazione finora
- Hypoalbuminemia - StatPearls - NCBI BookshelfDocumento6 pagineHypoalbuminemia - StatPearls - NCBI BookshelfAmin RaisNessuna valutazione finora
- What Everyone Should Know About AccutaneDocumento2 pagineWhat Everyone Should Know About AccutaneNur HazwaniNessuna valutazione finora
- Corona Virus InfographicDocumento1 paginaCorona Virus Infographicapi-510312435Nessuna valutazione finora
- Medicine MOMDocumento7 pagineMedicine MOMsushilshsNessuna valutazione finora
- Fetal DistressDocumento2 pagineFetal DistressLianne Joie Visitacion ClaroNessuna valutazione finora
- Genetic Disorders in Arab Populations: Qatar: Tawfeg Ben-Omran, Atqah Abdul WahabDocumento6 pagineGenetic Disorders in Arab Populations: Qatar: Tawfeg Ben-Omran, Atqah Abdul WahabUmair ZubairNessuna valutazione finora
- Gestational Diabetes Mellitus Case StudiesDocumento21 pagineGestational Diabetes Mellitus Case Studiesdiabetes asia100% (3)
- PDF Albumin Drug StudyDocumento1 paginaPDF Albumin Drug StudyJamie John EsplanadaNessuna valutazione finora
- Tropisetron 26Documento6 pagineTropisetron 26Tori SepriwanNessuna valutazione finora
- Appendix C: Nutrient Chart - Function, Deficiency and Toxicity Symptoms, and Major Food SourcesDocumento5 pagineAppendix C: Nutrient Chart - Function, Deficiency and Toxicity Symptoms, and Major Food SourcesMaria Christina LagartejaNessuna valutazione finora
- Doh Updated Prog M-RDocumento49 pagineDoh Updated Prog M-Rdeeday echavezNessuna valutazione finora
- Mental Health Awareness WorkbookDocumento50 pagineMental Health Awareness WorkbookpammiefisherNessuna valutazione finora
- Muscle Skeletal Trauma For EMSDocumento79 pagineMuscle Skeletal Trauma For EMSPaulhotvw67100% (4)
- DiphtheriaDocumento13 pagineDiphtheriaNiken AmritaNessuna valutazione finora
- Hardiness and Coping Strategies PDFDocumento18 pagineHardiness and Coping Strategies PDFadamiamNessuna valutazione finora
- Abdomen Pediatrics1Documento12 pagineAbdomen Pediatrics1cmalloupas91Nessuna valutazione finora