Potrebbero piacerti anche
- Cholinergics and AnticholinergicsDocumento5 pagineCholinergics and AnticholinergicscatislandbigredNessuna valutazione finora
- Electrolyte ImbalanceDocumento3 pagineElectrolyte ImbalancemewilkinNessuna valutazione finora
- Ninja - Anti-HTN PDFDocumento6 pagineNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Basic Principles of PharmacologyDocumento13 pagineBasic Principles of Pharmacologyemmanuel100% (1)
- Mishba +pharmacology + Tapan ShahDocumento232 pagineMishba +pharmacology + Tapan ShahRaushan BlakeNessuna valutazione finora
- Hmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, InteractionsDocumento6 pagineHmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, Interactionswaste78Nessuna valutazione finora
- Bmed Concept MapDocumento2 pagineBmed Concept Mapapi-247954649Nessuna valutazione finora
- Electrolyte Mnemonic QuizletDocumento3 pagineElectrolyte Mnemonic QuizletA.h.Murad100% (2)
- Pharmacology CNS DrugsDocumento15 paginePharmacology CNS DrugsM Youssif Elkady100% (1)
- Cardiovascular Pharmacology OutlineDocumento11 pagineCardiovascular Pharmacology OutlineLhay de OcampoNessuna valutazione finora
- OB Drug ChartsDocumento2 pagineOB Drug ChartsNursingSchoolNotesNessuna valutazione finora
- H Hemolysis E Elevated L Liver Function L Low P Platelet B Breast U Uterus B Bowel B Bladder L Lochia E Episiotomy H HemorrageDocumento7 pagineH Hemolysis E Elevated L Liver Function L Low P Platelet B Breast U Uterus B Bowel B Bladder L Lochia E Episiotomy H HemorrageAlexNessuna valutazione finora
- Antianginal DrugsDocumento3 pagineAntianginal DrugsyukariNessuna valutazione finora
- DRUGS Flash CardsDocumento9 pagineDRUGS Flash Cardsdrp2011Nessuna valutazione finora
- Pharmacology FirecrackerDocumento37 paginePharmacology FirecrackerRehan Usman100% (1)
- Comprehensive Pharmacology Study NotesDocumento123 pagineComprehensive Pharmacology Study NotesEdil M Jama100% (1)
- Drug ChartDocumento8 pagineDrug Chartstudentalwaysstudy100% (1)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDa EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNessuna valutazione finora
- Ninja - Cholinergic Drugs PDFDocumento4 pagineNinja - Cholinergic Drugs PDFErica Hyeyeon Lee100% (2)
- Template Drug Card1Documento1 paginaTemplate Drug Card1Kay TaylorNessuna valutazione finora
- Anti-Arrhythmic Agents For Pharmacy PDFDocumento41 pagineAnti-Arrhythmic Agents For Pharmacy PDFKelvinTMaikanaNessuna valutazione finora
- NSAIDS and SteroidsDocumento2 pagineNSAIDS and Steroidsmed testNessuna valutazione finora
- Cardiovascular Drugs XL ChartDocumento4 pagineCardiovascular Drugs XL Chartcdp158767% (3)
- Receptor Pharmacology Cheat Sheet (4f6203b546fa5)Documento5 pagineReceptor Pharmacology Cheat Sheet (4f6203b546fa5)sinthreckNessuna valutazione finora
- Grapefruit Juice and Drug Interactions - 0717Documento2 pagineGrapefruit Juice and Drug Interactions - 0717Asri YaniNessuna valutazione finora
- Pathophysiology of Endocrine SystemDocumento64 paginePathophysiology of Endocrine SystemTess MohamedNessuna valutazione finora
- Pharmacology Notes (Chapter 20 and 21)Documento2 paginePharmacology Notes (Chapter 20 and 21)graycorypNessuna valutazione finora
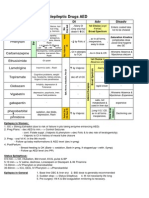
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocumento1 paginaAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Nessuna valutazione finora
- Autonomic DrugsDocumento107 pagineAutonomic DrugsMaria Mercedes LeivaNessuna valutazione finora
- O Insert Picture Here From Slide: Heart Failure Heart FailureDocumento4 pagineO Insert Picture Here From Slide: Heart Failure Heart FailureAlec Xavier MirandaNessuna valutazione finora
- Endocrine DisordersDocumento5 pagineEndocrine DisordersBilly Ray VillanuevaNessuna valutazione finora
- Ninja - Autacoids PDFDocumento3 pagineNinja - Autacoids PDFErica Hyeyeon LeeNessuna valutazione finora
- Agents Causing Coma or SeizuresDocumento3 pagineAgents Causing Coma or SeizuresShaira Aquino VerzosaNessuna valutazione finora
- ENDOCRINE NURSING-FINAL HDDocumento15 pagineENDOCRINE NURSING-FINAL HDJayvee Novenario Casaljay100% (1)
- Electrolytes ImbalancesDocumento4 pagineElectrolytes ImbalancesPeter John Ruiz100% (1)
- Opioids PDFDocumento2 pagineOpioids PDFErica Hyeyeon LeeNessuna valutazione finora
- Onco PharmacologyDocumento9 pagineOnco Pharmacologyarn0ld21Nessuna valutazione finora
- Cholinergics and Cholinergic BlockersDocumento5 pagineCholinergics and Cholinergic Blockersapi-3739910100% (3)
- NERVOUS MnemonicsDocumento4 pagineNERVOUS MnemonicsHimNessuna valutazione finora
- Cholinergic Drug MnemonicsDocumento1 paginaCholinergic Drug Mnemonicssunshine151100% (1)
- Common Drug Stems Cheat Sheet: Drug Stem Drug Class And/or Stem Explanation ExamplesDocumento2 pagineCommon Drug Stems Cheat Sheet: Drug Stem Drug Class And/or Stem Explanation ExamplesjthsNessuna valutazione finora
- Diabetes Treatment: PancreatitisDocumento2 pagineDiabetes Treatment: PancreatitisSafiya JamesNessuna valutazione finora
- CholestyramineDocumento1 paginaCholestyramineKatie McPeekNessuna valutazione finora
- FAELDONEA - B. Concept MapDocumento1 paginaFAELDONEA - B. Concept MapPatricia Jean FaeldoneaNessuna valutazione finora
- Musculoskeletal PharmacologyDocumento18 pagineMusculoskeletal PharmacologyBLEEMAGE100% (2)
- Nursing Pharmacology Inflammation Study GuideDocumento11 pagineNursing Pharmacology Inflammation Study GuideChelsea Smith100% (1)
- Ninja - Anemias PDFDocumento1 paginaNinja - Anemias PDFErica Hyeyeon LeeNessuna valutazione finora
- Cardiac Drugs HypertensionDocumento5 pagineCardiac Drugs HypertensionEciOwnsMeNessuna valutazione finora
- LasixDocumento1 paginaLasixKatie McPeek100% (2)
- Hormones and Related DrugsDocumento42 pagineHormones and Related DrugsRamya PrabhuNessuna valutazione finora
- PharmacologyDocumento35 paginePharmacologyJan Michael ArtiagaNessuna valutazione finora
- Endocrine DisordersDocumento27 pagineEndocrine Disordersasdfgrttt100% (4)
- Fluids and ElectrolytesDocumento9 pagineFluids and ElectrolytesAlvin Jay DacilloNessuna valutazione finora
- EndocrineDocumento2 pagineEndocrineUnclePorkchopNessuna valutazione finora
- Summary of Adrenergic DrugsDocumento3 pagineSummary of Adrenergic DrugsrabduljabarrNessuna valutazione finora
- Dysrhythmias Cheat SheetDocumento2 pagineDysrhythmias Cheat SheetKandice ChandlerNessuna valutazione finora
- Ninja - Antihyperlipidemics PDFDocumento3 pagineNinja - Antihyperlipidemics PDFErica Hyeyeon Lee100% (1)
- Anticholinergic: Anticholinergics: Generic and Brand NamesDocumento6 pagineAnticholinergic: Anticholinergics: Generic and Brand NamesSaffery Gly LayuganNessuna valutazione finora
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDocumento41 pagineDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityredderdatNessuna valutazione finora
- 7 - Cholinomimetic DrugsDocumento50 pagine7 - Cholinomimetic DrugslalitrajindoliaNessuna valutazione finora
- Corelation of The Changes Between The Iridocorneal - Angle and Other Paramet E Rs at The Neovascular GlaucomaDocumento25 pagineCorelation of The Changes Between The Iridocorneal - Angle and Other Paramet E Rs at The Neovascular GlaucomaAJVAZI100% (1)
- hdf492 Portfolio PresentationDocumento14 paginehdf492 Portfolio Presentationapi-403412647Nessuna valutazione finora
- Heart PDFDocumento48 pagineHeart PDFdr.chetan2385Nessuna valutazione finora
- CSR Activities - Hygiene and SanitationDocumento14 pagineCSR Activities - Hygiene and SanitationFinplus IndiaNessuna valutazione finora
- Child Safety PDFDocumento240 pagineChild Safety PDFVaibhav AgarwalNessuna valutazione finora
- Soal Bahasa Inggris SBMPTN 2003Documento3 pagineSoal Bahasa Inggris SBMPTN 2003soe_barn64Nessuna valutazione finora
- Syllabus FOR: AIAPGET 2023Documento5 pagineSyllabus FOR: AIAPGET 2023Rahul KirkNessuna valutazione finora
- Microbiology at A GlanceDocumento126 pagineMicrobiology at A GlanceMuhammad UsmanNessuna valutazione finora
- How To Use Akpi Seed For Hips, Butts and Breasts EnlargementDocumento5 pagineHow To Use Akpi Seed For Hips, Butts and Breasts EnlargementLinda PrideNessuna valutazione finora
- Clinical Neuroscience Psychopathology and The Brain 2Nd Edition Full ChapterDocumento41 pagineClinical Neuroscience Psychopathology and The Brain 2Nd Edition Full Chapterwilliam.kellar832100% (20)
- Philippine Navy Naval Installation Command Naval Installation and Facilities-National Capital RegionDocumento9 paginePhilippine Navy Naval Installation Command Naval Installation and Facilities-National Capital RegionDuchesne San JoseNessuna valutazione finora
- Desain GTSL SangryDocumento53 pagineDesain GTSL SangrySanggry Mutiara PardedeNessuna valutazione finora
- TDSB GR 9-12 Student Census, 2022Documento31 pagineTDSB GR 9-12 Student Census, 2022True NorthNessuna valutazione finora
- Technology and Its Negativity: English For Academic and Professional Purposes Performance Task 2: Position PaperDocumento2 pagineTechnology and Its Negativity: English For Academic and Professional Purposes Performance Task 2: Position PaperAlliah MatozaNessuna valutazione finora
- Estethic DentistreDocumento639 pagineEstethic DentistreAdrian Venegas Melo100% (1)
- BIO210 Infomation 7Documento5 pagineBIO210 Infomation 7Rex BrazilNessuna valutazione finora
- Critical Movie Review Template # 1: General InstructionsDocumento3 pagineCritical Movie Review Template # 1: General InstructionsNicole MilanNessuna valutazione finora
- Google Forms Survey Sample H.S.B SBA 2023Documento8 pagineGoogle Forms Survey Sample H.S.B SBA 2023Brianna ChuramanNessuna valutazione finora
- Health 7: Learner'S Instructional MaterialDocumento14 pagineHealth 7: Learner'S Instructional MaterialGeneNessuna valutazione finora
- COMSECXDocumento5 pagineCOMSECXJoseph CruzNessuna valutazione finora
- Rpms Evaluation For School Head (Mov'S / Mfo'S)Documento5 pagineRpms Evaluation For School Head (Mov'S / Mfo'S)Laiza Niña Gimenez LariegoNessuna valutazione finora
- Learner DiversityDocumento1 paginaLearner DiversityHenry Buemio100% (1)
- Memorandum: Philippine National Police Training Institute Regional Training Center 8Documento2 pagineMemorandum: Philippine National Police Training Institute Regional Training Center 8DUN SAMMUEL LAURENTENessuna valutazione finora
- Ketones &ketone Urine Test - Purpose, Procedure, ResutlsDocumento6 pagineKetones &ketone Urine Test - Purpose, Procedure, ResutlsEiann Jasper LongcayanaNessuna valutazione finora
- Review Jurnal Bunga Aurelia (18621005)Documento3 pagineReview Jurnal Bunga Aurelia (18621005)bungaNessuna valutazione finora
- Borderline and Histrionic Personality DisordersDocumento38 pagineBorderline and Histrionic Personality DisordersSahel100% (1)
- Pola 2017Documento10 paginePola 2017RobertoNessuna valutazione finora
- Paridhi English LanguageDocumento7 pagineParidhi English LanguageKasturi GhoshNessuna valutazione finora
- MS Civil Engineering Construction and Safety Management Assignment No. 1 MCE191010 Abdur RehmanDocumento5 pagineMS Civil Engineering Construction and Safety Management Assignment No. 1 MCE191010 Abdur RehmanAbdur RehmanNessuna valutazione finora
- Respect in The Workplace: The Management of Disrespectful ConductDocumento8 pagineRespect in The Workplace: The Management of Disrespectful ConductHP w1907Nessuna valutazione finora