Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Mil PRF 46010FDocumento20 pagineMil PRF 46010FSantaj Technologies100% (1)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Art of Communication PDFDocumento3 pagineThe Art of Communication PDFHung Tran JamesNessuna valutazione finora
- Gert-Jan Van Der Heiden - 'The Voice of Misery - A Continental Philosophy of Testimony' PDFDocumento352 pagineGert-Jan Van Der Heiden - 'The Voice of Misery - A Continental Philosophy of Testimony' PDFscottbrodieNessuna valutazione finora
- OCFINALEXAM2019Documento6 pagineOCFINALEXAM2019DA FT100% (1)
- Community Tax Certificate PRINTDocumento2 pagineCommunity Tax Certificate PRINTClarenz0% (1)
- Republic of Indonesia's Sovereign Immunity Upheld in Contract DisputeDocumento2 pagineRepublic of Indonesia's Sovereign Immunity Upheld in Contract DisputeEllis Lagasca100% (2)
- Quiz 1Documento6 pagineQuiz 1Eliza Mae Aquino100% (1)
- Tthe Sacrament of Reconciliation1Documento47 pagineTthe Sacrament of Reconciliation1Rev. Fr. Jessie Somosierra, Jr.Nessuna valutazione finora
- Exam 2 Study GuideDocumento11 pagineExam 2 Study GuideAnonymous ewJy7jyvNNessuna valutazione finora
- User Manual FotonaDocumento103 pagineUser Manual Fotonarasheeque100% (3)
- A.A AntagonismDocumento19 pagineA.A Antagonismjraj030_2k6Nessuna valutazione finora
- 2017 KGSP-G Application Guidelines (English)Documento42 pagine2017 KGSP-G Application Guidelines (English)Skolastika Christy RosariNessuna valutazione finora
- Review: Prevention and Treatment of The Common Cold: Making Sense of The EvidenceDocumento10 pagineReview: Prevention and Treatment of The Common Cold: Making Sense of The EvidenceRismayantiNessuna valutazione finora
- Trouble MeDocumento5 pagineTrouble MeRismayantiNessuna valutazione finora
- B1A4 - What's Going OnDocumento0 pagineB1A4 - What's Going Onnina9490Nessuna valutazione finora
- Kotliar Natalia Ja Sampio NooraDocumento32 pagineKotliar Natalia Ja Sampio NooraRismayantiNessuna valutazione finora
- FTP PDFDocumento5 pagineFTP PDFRismayantiNessuna valutazione finora
- JURJDocumento15 pagineJURJRismayantiNessuna valutazione finora
- 3916 19912 1 PBDocumento12 pagine3916 19912 1 PBRismayantiNessuna valutazione finora
- Ann Rheum Dis 2015 Singh 631 4Documento5 pagineAnn Rheum Dis 2015 Singh 631 4RismayantiNessuna valutazione finora
- AJAN 25-3 PeartDocumento6 pagineAJAN 25-3 PeartRismayantiNessuna valutazione finora
- 89 1458069050 PDFDocumento7 pagine89 1458069050 PDFRismayantiNessuna valutazione finora
- Preventing Pressure Ulcers in People With Spinal.8Documento10 paginePreventing Pressure Ulcers in People With Spinal.8RismayantiNessuna valutazione finora
- Hepatocellular Carcinoma Liver CancerDocumento11 pagineHepatocellular Carcinoma Liver CancerRismayantiNessuna valutazione finora
- 2002JNeurosurgAnesth14 50Documento6 pagine2002JNeurosurgAnesth14 50RismayantiNessuna valutazione finora
- Article 3106277287Documento11 pagineArticle 3106277287RismayantiNessuna valutazione finora
- Promise: (Music Video Spoken Part:)Documento5 paginePromise: (Music Video Spoken Part:)RismayantiNessuna valutazione finora
- ExoDocumento16 pagineExoRismayantiNessuna valutazione finora
- Micronutrieint Loss ObeseDocumento10 pagineMicronutrieint Loss ObeseYazen JoudehNessuna valutazione finora
- Value Creation-How-Can-The-Semiconductor-Industry-Keep-Outperforming-FinalDocumento7 pagineValue Creation-How-Can-The-Semiconductor-Industry-Keep-Outperforming-FinalJoão Vitor RibeiroNessuna valutazione finora
- MEPQ7202 Security OfficerDocumento55 pagineMEPQ7202 Security OfficerSALMANNessuna valutazione finora
- B1 Grammar and VocabularyDocumento224 pagineB1 Grammar and VocabularyTranhylapNessuna valutazione finora
- Doubles and Doppelgangers: Religious Meaning For The Young and OldDocumento12 pagineDoubles and Doppelgangers: Religious Meaning For The Young and Old0 1Nessuna valutazione finora
- F77 - Service ManualDocumento120 pagineF77 - Service ManualStas MNessuna valutazione finora
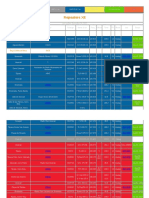
- Repeaters XE PDFDocumento12 pagineRepeaters XE PDFenzzo molinariNessuna valutazione finora
- PB13MAT - 13 Project Stakeholder ManagementDocumento30 paginePB13MAT - 13 Project Stakeholder ManagementYudhi ChristianNessuna valutazione finora
- Stakeholder Management Plan Case Study 1Documento2 pagineStakeholder Management Plan Case Study 1Krister VallenteNessuna valutazione finora
- Innovations in Teaching-Learning ProcessDocumento21 pagineInnovations in Teaching-Learning ProcessNova Rhea GarciaNessuna valutazione finora
- ĐỀ MINH HỌA 15-19Documento25 pagineĐỀ MINH HỌA 15-19Trung Vũ ThànhNessuna valutazione finora
- Manoj KR - KakatiDocumento5 pagineManoj KR - Kakatimanoj kakatiNessuna valutazione finora
- What are plot pointsDocumento19 pagineWhat are plot pointsOpeeron OpeeNessuna valutazione finora
- Effect of Disinfectants On Highly Pathogenic Avian in Uenza Virus (H5N1) in Lab and Poultry FarmsDocumento7 pagineEffect of Disinfectants On Highly Pathogenic Avian in Uenza Virus (H5N1) in Lab and Poultry FarmsBalvant SinghNessuna valutazione finora
- ICE Professional Review GuidanceDocumento23 pagineICE Professional Review Guidancerahulgehlot2008Nessuna valutazione finora
- David Emmett & Graeme Nice - What You Need To Know About Cannabis - Understanding The FactsDocumento120 pagineDavid Emmett & Graeme Nice - What You Need To Know About Cannabis - Understanding The FactsJovana StojkovićNessuna valutazione finora
- Economics 1A and B WorkbookDocumento90 pagineEconomics 1A and B WorkbookmrlsrpssqbucxwswfjNessuna valutazione finora
- Integrating Force - Com With MicrosoftDocumento11 pagineIntegrating Force - Com With MicrosoftSurajAluruNessuna valutazione finora
- Colorectal Disease - 2023 - Freund - Can Preoperative CT MR Enterography Preclude The Development of Crohn S Disease LikeDocumento10 pagineColorectal Disease - 2023 - Freund - Can Preoperative CT MR Enterography Preclude The Development of Crohn S Disease Likedavidmarkovic032Nessuna valutazione finora
- Chapter 2 Phil. HistoryDocumento4 pagineChapter 2 Phil. HistoryJaylene AlbayNessuna valutazione finora