Potrebbero piacerti anche
- LANCET 12-Citicolina (Somazina) en Tratamiento de Ictus IsquemicoDocumento9 pagineLANCET 12-Citicolina (Somazina) en Tratamiento de Ictus IsquemicorhymescsfNessuna valutazione finora
- Citicoline For CognitiveDocumento7 pagineCiticoline For CognitiveSyafrie YunizarNessuna valutazione finora
- CC 12031Documento200 pagineCC 12031Arti Tyagita KusumawardhaniNessuna valutazione finora
- Research ArticleDocumento13 pagineResearch ArticleJames Cojab SacalNessuna valutazione finora
- 30 Muninathan EtalDocumento6 pagine30 Muninathan EtaleditorijmrhsNessuna valutazione finora
- PHD Thesis: University of Medicine and Pharmacy CraiovaDocumento10 paginePHD Thesis: University of Medicine and Pharmacy CraiovapaulNessuna valutazione finora
- Regenerative Therapies For Equine Degenerative Joint Disease: A Preliminary StudyDocumento11 pagineRegenerative Therapies For Equine Degenerative Joint Disease: A Preliminary StudyCarlos Alberto CastañedaNessuna valutazione finora
- Transplant International Special Issue: Abstracts of The 14th Congress of The European Society For Organ Transplantation Volume 22, Issue Supplement s2, Pages 95-222, August 2009Documento128 pagineTransplant International Special Issue: Abstracts of The 14th Congress of The European Society For Organ Transplantation Volume 22, Issue Supplement s2, Pages 95-222, August 2009Enrique Moreno GonzálezNessuna valutazione finora
- Clinical Nutrition: Original ArticleDocumento6 pagineClinical Nutrition: Original ArticleS Dian RNessuna valutazione finora
- CiticolineDocumento18 pagineCiticolineJennifer BryantNessuna valutazione finora
- AgeLOC Vitality CompendiumDocumento16 pagineAgeLOC Vitality CompendiumElements OfyouthNessuna valutazione finora
- FluidDocumento190 pagineFluidAndrias OzNessuna valutazione finora
- 9 Randomized Phase III Evaluation of Cisplatin PlusDocumento6 pagine9 Randomized Phase III Evaluation of Cisplatin Plustrifamonika23Nessuna valutazione finora
- Revision CiticolinaDocumento20 pagineRevision CiticolinaIhdhar NursNessuna valutazione finora
- CiticolinaDocumento13 pagineCiticolinaCarlos PalominoNessuna valutazione finora
- Adrenal Insufficiency in Thyroid Cancer Patients Treated With Tyrosine Kinase Inhibitors and Detected by ACTH Stimulation TestDocumento9 pagineAdrenal Insufficiency in Thyroid Cancer Patients Treated With Tyrosine Kinase Inhibitors and Detected by ACTH Stimulation TestEmanuel CalderonNessuna valutazione finora
- Pi Is 1474442213700371Documento7 paginePi Is 1474442213700371hubik38Nessuna valutazione finora
- Focus: Efficacy of Riluzole in The Treatment of Spinal Cord Injury: A Systematic Review of The LiteratureDocumento18 pagineFocus: Efficacy of Riluzole in The Treatment of Spinal Cord Injury: A Systematic Review of The LiteratureAna Flávia ResendeNessuna valutazione finora
- Changes in Cytokine Production in Healthy Subjects Practicing Guolin Qigong: A Pilot StudyDocumento7 pagineChanges in Cytokine Production in Healthy Subjects Practicing Guolin Qigong: A Pilot StudyThiago NunesNessuna valutazione finora
- Physiology PharmacologyDocumento126 paginePhysiology PharmacologyuneedlesNessuna valutazione finora
- GinsengDocumento7 pagineGinsengMarcela Catalina Fandiño VargasNessuna valutazione finora
- Jurnal TMKDocumento10 pagineJurnal TMKvanilla wottledNessuna valutazione finora
- 8 HalamansdbDocumento14 pagine8 HalamansdbbanglarkNessuna valutazione finora
- Journal Pone 0269224Documento12 pagineJournal Pone 0269224Bayu AndiNessuna valutazione finora
- Out 41Documento12 pagineOut 41natanatalisNessuna valutazione finora
- Hydroxychloroquine Effects On Mir-155-3P and Mir-219 Expression Changes in Animal Model of Multiple SclerosisDocumento9 pagineHydroxychloroquine Effects On Mir-155-3P and Mir-219 Expression Changes in Animal Model of Multiple SclerosisAlvesnigelNessuna valutazione finora
- Cardiovascular Risk in Clopidogrel-Treated Patients According To Cytochrome P450 2C19 2 Loss-of-Function Allele or Proton Pump Inhibitor CoadministrationDocumento10 pagineCardiovascular Risk in Clopidogrel-Treated Patients According To Cytochrome P450 2C19 2 Loss-of-Function Allele or Proton Pump Inhibitor CoadministrationVenansius ReinaldiNessuna valutazione finora
- Background: ISRCTN34716921Documento5 pagineBackground: ISRCTN34716921Sav GaNessuna valutazione finora
- Expresion of GLP1 in Thyroid CarcinomaDocumento9 pagineExpresion of GLP1 in Thyroid CarcinomaW Antonio Rivera MartínezNessuna valutazione finora
- Glutamina IVDocumento11 pagineGlutamina IVBLADIMIR ALEJANDRO GIL VALENCIANessuna valutazione finora
- Nej Mo A 0804328Documento12 pagineNej Mo A 0804328agniajolandaNessuna valutazione finora
- Song 2014Documento11 pagineSong 2014Ayssa WitjaksonoNessuna valutazione finora
- Fungi & Cancer TherapyDocumento18 pagineFungi & Cancer TherapyLynn McdonaldNessuna valutazione finora
- Clinical Study: Obesity and Cytokines in Childhood-Onset Systemic Lupus ErythematosusDocumento6 pagineClinical Study: Obesity and Cytokines in Childhood-Onset Systemic Lupus ErythematosusIndra KusumayadiNessuna valutazione finora
- ParlakDocumento10 pagineParlakARFANNessuna valutazione finora
- The Use of Sildenafil in Persistent Pulmonary Hypertension of The Newborn PDFDocumento6 pagineThe Use of Sildenafil in Persistent Pulmonary Hypertension of The Newborn PDFmaciasdrNessuna valutazione finora
- Adipokines and Systemic Inflammation in Weight-Losing Lung Cancer PatientsDocumento6 pagineAdipokines and Systemic Inflammation in Weight-Losing Lung Cancer PatientsAnna GozaliNessuna valutazione finora
- Jover JC PEGfilgrastimDocumento7 pagineJover JC PEGfilgrastimCheli GarciaNessuna valutazione finora
- MD 1 Section E2 Group 3 Biochem REVISEDDocumento10 pagineMD 1 Section E2 Group 3 Biochem REVISEDParadoxistNessuna valutazione finora
- Complementary Therapies in Clinical PracticeDocumento9 pagineComplementary Therapies in Clinical PracticeKurnia NuriNessuna valutazione finora
- Biochem Journal CritiqueDocumento7 pagineBiochem Journal CritiqueDiane TomogbongNessuna valutazione finora
- Assessment of Quality of Life in A Double-Blind, Randomized Clinical Trial of Imidapril and Captopril For Hypertensive Chinese in TaiwanDocumento7 pagineAssessment of Quality of Life in A Double-Blind, Randomized Clinical Trial of Imidapril and Captopril For Hypertensive Chinese in TaiwanSherllen ChandraNessuna valutazione finora
- A Phase III Study of Siltumaximab (CNTO 328) Anti Interleukin 6 Monoclonal Antibody in Metastatic Renal Cell Cancer.2010Documento9 pagineA Phase III Study of Siltumaximab (CNTO 328) Anti Interleukin 6 Monoclonal Antibody in Metastatic Renal Cell Cancer.2010Fina Herlinda NurNessuna valutazione finora
- PrintDocumento8 paginePrintannarchyNessuna valutazione finora
- Postnatal Hydrocortisone For Preventing or Treating Bronchopulmonary Dysplasia in Preterm Infants: A Systematic ReviewDocumento7 paginePostnatal Hydrocortisone For Preventing or Treating Bronchopulmonary Dysplasia in Preterm Infants: A Systematic ReviewAldy RinaldiNessuna valutazione finora
- Current Therapeutic ResearchDocumento6 pagineCurrent Therapeutic ResearchVincent ReyesNessuna valutazione finora
- Comparable Efficacy and Safety of Generic Imatinib and Branded Imatinib in Patients With Newly Diagnosed Chronic Myeloid LeukaemiaDocumento39 pagineComparable Efficacy and Safety of Generic Imatinib and Branded Imatinib in Patients With Newly Diagnosed Chronic Myeloid Leukaemiarisna sariNessuna valutazione finora
- Cerebrolysin Increases Recovery and Decreases Inflammation in An Autoimmune Model of Autoimmune EncephalitisDocumento15 pagineCerebrolysin Increases Recovery and Decreases Inflammation in An Autoimmune Model of Autoimmune EncephalitisAlin MihaiNessuna valutazione finora
- Gene Therapy For Type 1 Diabetes Mellitus in Rats by Gastrointestinal Administration of Chitosan Nanoparticles Containing Human Insulin GeneDocumento7 pagineGene Therapy For Type 1 Diabetes Mellitus in Rats by Gastrointestinal Administration of Chitosan Nanoparticles Containing Human Insulin GenesaifudinNessuna valutazione finora
- Theobromine Inhibits CoughDocumento16 pagineTheobromine Inhibits CoughRaffaello MobiliaNessuna valutazione finora
- Clinical Course of Steroid Sensitive Nephrotic Syndrome in Children: Outcome and OutlookDocumento11 pagineClinical Course of Steroid Sensitive Nephrotic Syndrome in Children: Outcome and OutlookIkhbar FalahNessuna valutazione finora
- Current Therapeutic Advances in Chronic Interstitial CystitisDocumento8 pagineCurrent Therapeutic Advances in Chronic Interstitial CystitisYylfordt GranzNessuna valutazione finora
- Evidence-Based Treatmentsin Pemphigusvulgaris Andpemphigus FoliaceusDocumento8 pagineEvidence-Based Treatmentsin Pemphigusvulgaris Andpemphigus FoliaceusCharly EscobarNessuna valutazione finora
- Corticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisDocumento7 pagineCorticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisshiloinNessuna valutazione finora
- Cupping For Patients With Inflammatory CDocumento2 pagineCupping For Patients With Inflammatory CPatryk StowaszewskiNessuna valutazione finora
- JCO 2005 Low 2726 34Documento9 pagineJCO 2005 Low 2726 34Donny Artya KesumaNessuna valutazione finora
- Paper Title: (16 Bold Blue Color)Documento9 paginePaper Title: (16 Bold Blue Color)Fauzi RusdiantoNessuna valutazione finora
- ACD856, A Novel Positive Allosteric Modulator of TRK Receptors, Single Ascending Doses in Healthy Subjects: Safety and PharmacokineticsDocumento11 pagineACD856, A Novel Positive Allosteric Modulator of TRK Receptors, Single Ascending Doses in Healthy Subjects: Safety and PharmacokineticsMichael UNessuna valutazione finora
- DD Iicc AA: Use of Protein C Concentrate in Pediatric Patients With SepsisDocumento6 pagineDD Iicc AA: Use of Protein C Concentrate in Pediatric Patients With SepsisAlvin Brilian BudionoNessuna valutazione finora
- Complementary and Alternative Medical Lab Testing Part 8: UrologyDa EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyValutazione: 3 su 5 stelle3/5 (1)
- Module 14 Pediatric TB ENGLISHDocumento85 pagineModule 14 Pediatric TB ENGLISHDellNessuna valutazione finora
- 5 Morisky Medication Adherence-Scale PDFDocumento1 pagina5 Morisky Medication Adherence-Scale PDFDellNessuna valutazione finora
- Family Planning HandbookDocumento387 pagineFamily Planning HandbookvthiseasNessuna valutazione finora
- Jurnal Farmakologi Anti Konvulsi PDFDocumento13 pagineJurnal Farmakologi Anti Konvulsi PDFtherempongss100% (1)
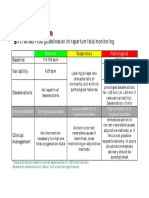
- CTG Classification PDFDocumento1 paginaCTG Classification PDFDellNessuna valutazione finora
- 5 Morisky Medication Adherence-Scale PDFDocumento1 pagina5 Morisky Medication Adherence-Scale PDFDellNessuna valutazione finora
- SPSS Crosstab PDFDocumento3 pagineSPSS Crosstab PDFDellNessuna valutazione finora
- A Practical Classification of Septonasal Deviation.42Documento3 pagineA Practical Classification of Septonasal Deviation.42DellNessuna valutazione finora
- Fitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDocumento30 pagineFitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDellNessuna valutazione finora
- Appendix 8 Normal Urine Output PDFDocumento1 paginaAppendix 8 Normal Urine Output PDFDellNessuna valutazione finora
- Cutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDocumento10 pagineCutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDellNessuna valutazione finora
- Complaints and Recalls HandlingDocumento50 pagineComplaints and Recalls HandlingSandraNessuna valutazione finora
- Carbohydrates Part 4Documento46 pagineCarbohydrates Part 4Frnckk MnstrNessuna valutazione finora
- Standards of Psychiatric-Mental Health Nursing PracticeDocumento4 pagineStandards of Psychiatric-Mental Health Nursing PracticeAnna Sofia ReyesNessuna valutazione finora
- Treating The Mother of Black Triangles With Bioclear VeneersDocumento4 pagineTreating The Mother of Black Triangles With Bioclear VeneersThe Bioclear ClinicNessuna valutazione finora
- Csa - Rams Top Tips Part 1Documento7 pagineCsa - Rams Top Tips Part 1Zaheer AliNessuna valutazione finora
- Zenon Research PaperDocumento1 paginaZenon Research PaperZenon PalomaNessuna valutazione finora
- Multiple IV Bolus AdministrationDocumento21 pagineMultiple IV Bolus AdministrationIka NurzijahNessuna valutazione finora
- Atopic Dermatitis and HomoeopathyDocumento8 pagineAtopic Dermatitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Into To Balance Method ImagingDocumento8 pagineInto To Balance Method ImagingSkorman7Nessuna valutazione finora
- Nursing InformaticsDocumento5 pagineNursing InformaticsDanica BonNessuna valutazione finora
- Full Elc 25-5Documento51 pagineFull Elc 25-5zone100% (2)
- Dechlorination of WaterDocumento4 pagineDechlorination of WaterByaruhanga EmmanuelNessuna valutazione finora
- Hydrocephalus: I Dewa Ketut Gede Herry Oka Pembimbing: Dr. Dr. I Wayan Niryana, Sp. BS (K)Documento40 pagineHydrocephalus: I Dewa Ketut Gede Herry Oka Pembimbing: Dr. Dr. I Wayan Niryana, Sp. BS (K)Dewa Oka100% (1)
- Basic Hypnotherapy Steve G Jones EbookDocumento176 pagineBasic Hypnotherapy Steve G Jones EbookElias Calix87% (15)
- Understanding Eating DisordersDocumento10 pagineUnderstanding Eating DisorderspuchioNessuna valutazione finora
- Đề cương nội nha rte manhDocumento24 pagineĐề cương nội nha rte manhMai Anh NguyenNessuna valutazione finora
- Annex A.1 Sample RLE Learning PlansDocumento2 pagineAnnex A.1 Sample RLE Learning PlansChevelle Valenciano-GaanNessuna valutazione finora
- Meditation With Yoga, Group Therapy With Hypnosis, and Psychoeducation For Long-Term Depressed Mood: A Randomized Pilot TrialDocumento16 pagineMeditation With Yoga, Group Therapy With Hypnosis, and Psychoeducation For Long-Term Depressed Mood: A Randomized Pilot TrialAnonymous 6h9W2AeSCNessuna valutazione finora
- Drug Study. GeamhDocumento5 pagineDrug Study. GeamhMacky RobentaNessuna valutazione finora
- DR Martine Faure Alderson - Cranio Sacral Reflexology Is BornDocumento3 pagineDR Martine Faure Alderson - Cranio Sacral Reflexology Is BornCatherine Smith100% (1)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocumento11 pagineAssessment Diagnosis Planning Intervention Rationale EvaluationDeo OlarteNessuna valutazione finora
- Freud Essay QuestionDocumento13 pagineFreud Essay Questionapi-315675568Nessuna valutazione finora
- DiazepamDocumento2 pagineDiazepamRochelle DiezmoNessuna valutazione finora
- Aga Spec 700040Documento18 pagineAga Spec 700040ryder3902Nessuna valutazione finora
- Drains and SewersDocumento13 pagineDrains and SewersAnil MishraNessuna valutazione finora
- AnsdDocumento22 pagineAnsdigorNessuna valutazione finora
- MJDF Mcqs - Mixed - PDFDocumento19 pagineMJDF Mcqs - Mixed - PDFAyesha Awan0% (3)
- ETDRSDocumento16 pagineETDRSAna Cecy AvalosNessuna valutazione finora
- AMT Balloon G Tube V5 Part Numbers and HCPCDocumento1 paginaAMT Balloon G Tube V5 Part Numbers and HCPCstarykNessuna valutazione finora