Potrebbero piacerti anche
- P 3 KDocumento23 pagineP 3 KlaudyaNessuna valutazione finora
- Jaeger ChartDocumento2 pagineJaeger ChartDavid Andres Cañas Suarez100% (1)
- Produk E-Katalog Lapi Berdasarkan Fornas Atau TidakDocumento7 pagineProduk E-Katalog Lapi Berdasarkan Fornas Atau TidaklaudyaNessuna valutazione finora
- Jadwal Sistri Versi 4Documento4 pagineJadwal Sistri Versi 4laudyaNessuna valutazione finora
- HydrotherapyDocumento8 pagineHydrotherapylaudyaNessuna valutazione finora
- Hydrotherapy techniquesDocumento8 pagineHydrotherapy techniqueslaudyaNessuna valutazione finora
- BingDocumento5 pagineBinglaudyaNessuna valutazione finora
- Endodontics EMADocumento3 pagineEndodontics EMAlaudyaNessuna valutazione finora
- Jadwal Kasman DLLDocumento2 pagineJadwal Kasman DLLlaudyaNessuna valutazione finora
- Big KelDocumento11 pagineBig KellaudyaNessuna valutazione finora
- Tugas EnglishDocumento1 paginaTugas EnglishlaudyaNessuna valutazione finora
- Jurnal FixDocumento7 pagineJurnal FixlaudyaNessuna valutazione finora
- Continuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress SyndromeDocumento4 pagineContinuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress Syndromelaudya100% (1)
- Introducing Pityriasis Rubra Pilaris (PRP) Refers To A Group of Chronic Disorders Characterized byDocumento1 paginaIntroducing Pityriasis Rubra Pilaris (PRP) Refers To A Group of Chronic Disorders Characterized bylaudyaNessuna valutazione finora
- Output SpssDocumento3 pagineOutput SpsslaudyaNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- TFN Declaration FormDocumento6 pagineTFN Declaration FormTim DunnNessuna valutazione finora
- Steps of Repertorization - 5e097dab9ad98Documento18 pagineSteps of Repertorization - 5e097dab9ad98Sowjanya JyothsnaNessuna valutazione finora
- ADA Design Guide 2010Documento7 pagineADA Design Guide 2010Jack BarkerNessuna valutazione finora
- Mri 7 TeslaDocumento12 pagineMri 7 TeslaJEAN FELLIPE BARROSNessuna valutazione finora
- Calculation of Lightning and Switching Overvoltages Transferred Through Power TransformerDocumento9 pagineCalculation of Lightning and Switching Overvoltages Transferred Through Power TransformerBožidar Filipović-GrčićNessuna valutazione finora
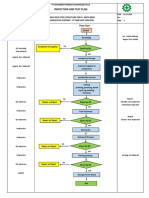
- Inspection and Test Plan: Flow Chart Start IncomingDocumento1 paginaInspection and Test Plan: Flow Chart Start IncomingSinden AyuNessuna valutazione finora
- Environmental Product Declaration: PU EuropeDocumento6 pagineEnvironmental Product Declaration: PU EuropeIngeniero Mac DonnellNessuna valutazione finora
- Earthing of GIS Type ELK - GTIDocumento20 pagineEarthing of GIS Type ELK - GTIJairo MoralesNessuna valutazione finora
- Requirement & Other Requirement: 2.311 Procedure For Accessing Applicable LegalDocumento2 pagineRequirement & Other Requirement: 2.311 Procedure For Accessing Applicable Legalkirandevi1981Nessuna valutazione finora
- Regulation of Body FluidsDocumento7 pagineRegulation of Body FluidsRuth FamillaranNessuna valutazione finora
- Holy Cross Academy Quarterly Cookery ExamDocumento4 pagineHoly Cross Academy Quarterly Cookery ExamAlle Eiram Padillo95% (21)
- Rajasthan PET Chemistry 1997 Exam with Detailed SolutionsDocumento34 pagineRajasthan PET Chemistry 1997 Exam with Detailed SolutionsYumit MorwalNessuna valutazione finora
- Charlotte's Web: SynopsisDocumento6 pagineCharlotte's Web: SynopsisAmbrosio MéndezNessuna valutazione finora
- Bio ViberDocumento7 pagineBio ViberMarco BuntNessuna valutazione finora
- Khatr Khola ISP District RatesDocumento56 pagineKhatr Khola ISP District RatesCivil EngineeringNessuna valutazione finora
- Lecture 1 Biochem 232 CellsDocumento13 pagineLecture 1 Biochem 232 CellsaelmowafyNessuna valutazione finora
- PGAU - BOHC2018-05 - 20pg - Lowres - Leader Cable AAC Conductor Data PDFDocumento20 paginePGAU - BOHC2018-05 - 20pg - Lowres - Leader Cable AAC Conductor Data PDFKelly chatNessuna valutazione finora
- Separation/Termination of Employment Policy SampleDocumento4 pagineSeparation/Termination of Employment Policy SampleferNessuna valutazione finora
- Chapter 2 Electronic StructureDocumento62 pagineChapter 2 Electronic StructureLivan TuahNessuna valutazione finora
- Catálogo SEDIVERDocumento32 pagineCatálogo SEDIVEREnver Rojas DiazNessuna valutazione finora
- Diploma Pharmacy First Year - Hap - MCQSDocumento13 pagineDiploma Pharmacy First Year - Hap - MCQSAnitha Mary Dambale91% (33)
- Limetas Maximos ResidualesDocumento27 pagineLimetas Maximos ResidualesXjoelx Olaya GonzalesNessuna valutazione finora
- The Turbo Air 6000 Centrifugal Compressor Handbook AAEDR-H-082 Rev 05 TA6000Documento137 pagineThe Turbo Air 6000 Centrifugal Compressor Handbook AAEDR-H-082 Rev 05 TA6000Rifki TriAditiya PutraNessuna valutazione finora
- Soil properties problemsDocumento2 pagineSoil properties problemsAldrin LampareroNessuna valutazione finora
- PR Cuisine vs US CuisineDocumento2 paginePR Cuisine vs US CuisineJannette HernandezNessuna valutazione finora
- Experiment Report Basic Physics "Total Internal Reflection"Documento10 pagineExperiment Report Basic Physics "Total Internal Reflection"dita wulanNessuna valutazione finora
- 4-Week Weight Loss ChallengeDocumento6 pagine4-Week Weight Loss ChallengeTammy JacksonNessuna valutazione finora
- Partial Defoliation of Vitis Vinifera L. Cv. Cabernet SauvignonDocumento9 paginePartial Defoliation of Vitis Vinifera L. Cv. Cabernet Sauvignon1ab4cNessuna valutazione finora
- The Pentester BlueprintDocumento27 pagineThe Pentester Blueprintjames smith100% (1)
- ABB Leaflet Comem BR-En 2018-06-07Documento2 pagineABB Leaflet Comem BR-En 2018-06-07Dave ChaudhuryNessuna valutazione finora