Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
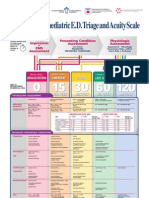
- Paediatric Triage PosterDocumento1 paginaPaediatric Triage PosterGenaro Olmos Garcia100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Indemnity Bond Form No.3762 To Get Duplicate LIC Policy Bond PDFDocumento2 pagineIndemnity Bond Form No.3762 To Get Duplicate LIC Policy Bond PDFPurushothama Rao Nalamati80% (10)
- Examen BLSDocumento6 pagineExamen BLSJYLM20980% (5)
- BLS Pretest AllDocumento8 pagineBLS Pretest AllTatianaGutuNessuna valutazione finora
- Bls Practice 1Documento4 pagineBls Practice 1Purushothama Rao NalamatiNessuna valutazione finora
- Uefa B AssignmentDocumento23 pagineUefa B AssignmentArnelaŠabanovićNessuna valutazione finora
- Musician's Handbook - 2016Documento132 pagineMusician's Handbook - 2016debikson0% (1)
- Kettlebell Secrets Special ReportDocumento10 pagineKettlebell Secrets Special Reportpopeyeballina78% (9)
- Extended Posteromedial Approach for Ankle FracturesDocumento87 pagineExtended Posteromedial Approach for Ankle FracturesPurushothama Rao NalamatiNessuna valutazione finora
- Approach - More Detail: Midfoot - Midfoot, Intertarsal FracturesDocumento12 pagineApproach - More Detail: Midfoot - Midfoot, Intertarsal FracturesPurushothama Rao NalamatiNessuna valutazione finora
- American Red Cross Hand BookDocumento74 pagineAmerican Red Cross Hand BookhafidzahNessuna valutazione finora
- Saudi CPR Guidlines in EnglishDocumento16 pagineSaudi CPR Guidlines in EnglishpiyushbamsNessuna valutazione finora
- Huckstep Nail For Periimplant FractureDocumento3 pagineHuckstep Nail For Periimplant FracturePurushothama Rao NalamatiNessuna valutazione finora
- 3 CPR 1Documento42 pagine3 CPR 1Ridho HidayatullohNessuna valutazione finora
- Three Column Fixation For Complex Proximal TibiaDocumento27 pagineThree Column Fixation For Complex Proximal TibiaPurushothama Rao NalamatiNessuna valutazione finora
- Presentation 1Documento13 paginePresentation 1Purushothama Rao NalamatiNessuna valutazione finora
- Posterior Coronal Plating of Bicondylar Tibial Plateau Fractures Through Posteromedial and Anterolateral Approaches in A Healthy Floating Supine PositionDocumento6 paginePosterior Coronal Plating of Bicondylar Tibial Plateau Fractures Through Posteromedial and Anterolateral Approaches in A Healthy Floating Supine PositionPurushothama Rao NalamatiNessuna valutazione finora
- Multiplate Recon of Severe Bicondylar FracDocumento5 pagineMultiplate Recon of Severe Bicondylar FracPurushothama Rao NalamatiNessuna valutazione finora
- Management Tibial Plateau FractureDocumento45 pagineManagement Tibial Plateau FracturePurushothama Rao NalamatiNessuna valutazione finora
- Multiplate Recon of Severe Bicondylar FracDocumento5 pagineMultiplate Recon of Severe Bicondylar FracPurushothama Rao NalamatiNessuna valutazione finora
- Clinical ExaminationDocumento7 pagineClinical ExaminationPurushothama Rao NalamatiNessuna valutazione finora
- Sto Indus Knee 2Documento59 pagineSto Indus Knee 2Purushothama Rao NalamatiNessuna valutazione finora
- Assessment Form AFO N KAFODocumento6 pagineAssessment Form AFO N KAFOrehanalisamoon112Nessuna valutazione finora
- Pes PlanusDocumento6 paginePes PlanusdeffyNessuna valutazione finora
- Foot Muscles ChartsDocumento6 pagineFoot Muscles ChartsddNessuna valutazione finora
- 5.56×45mm NATODocumento19 pagine5.56×45mm NATOJAIRNessuna valutazione finora
- Shoulder JointDocumento6 pagineShoulder JointDr santoshNessuna valutazione finora
- Scavenger Hunt-AnswersDocumento2 pagineScavenger Hunt-Answersapi-236445988Nessuna valutazione finora
- Hasang Hydro Power Plant Generates 275 GWh AnnuallyDocumento62 pagineHasang Hydro Power Plant Generates 275 GWh AnnuallyMark Jayson Baes NamucoNessuna valutazione finora
- Pain Modulation MechanismsDocumento10 paginePain Modulation Mechanismssmartie_chaiNessuna valutazione finora
- IHKS Summit ProgramDocumento35 pagineIHKS Summit ProgramDiah Rahayu SetiawatiNessuna valutazione finora
- RappellingDocumento114 pagineRappellingGaribaldi PerrusiNessuna valutazione finora
- Gait AssessmentDocumento71 pagineGait Assessmentelenita702100% (2)
- Dental Exam Questions on Conservative Dentistry and EndodonticsDocumento8 pagineDental Exam Questions on Conservative Dentistry and EndodonticsJude Aldo PaulNessuna valutazione finora
- Osteogenesis Imperfecta Power PointDocumento29 pagineOsteogenesis Imperfecta Power PointJonathan Jeffry Pratama100% (1)
- Atlas of Nerve Conduction Studies and Electromyography (2 Ed.)Documento10 pagineAtlas of Nerve Conduction Studies and Electromyography (2 Ed.)rodrigocorcino899959Nessuna valutazione finora
- Shortcut To Permanent DisabilityDocumento1 paginaShortcut To Permanent DisabilityGodfrey William MakileNessuna valutazione finora
- Vector D ModelsDocumento20 pagineVector D ModelsJose BurritoNessuna valutazione finora
- Pattern of Injuries in Fall From Height PDFDocumento4 paginePattern of Injuries in Fall From Height PDFRetno SawitriNessuna valutazione finora
- Ian 167/12Documento23 pagineIan 167/12babarkhattakNessuna valutazione finora
- Er Test DrillsDocumento26 pagineEr Test DrillsconinitasNessuna valutazione finora
- Bank Soalan MorfologiDocumento12 pagineBank Soalan MorfologiwiesukhihotuNessuna valutazione finora
- Belt Failure AnalysisDocumento8 pagineBelt Failure AnalysisDavid ChandlerNessuna valutazione finora
- FlipCutter A Pin That Changes Arthroscopic Tunnel Drilling Forever...Documento12 pagineFlipCutter A Pin That Changes Arthroscopic Tunnel Drilling Forever...andrelbportoNessuna valutazione finora
- Final Flight (OCR)Documento34 pagineFinal Flight (OCR)Andrés ArceNessuna valutazione finora
- O'Neal v. Food Lion Inc, 4th Cir. (1997)Documento4 pagineO'Neal v. Food Lion Inc, 4th Cir. (1997)Scribd Government DocsNessuna valutazione finora
- Aerial Lift Safety: Weekly ES&H Toolbox TalkDocumento1 paginaAerial Lift Safety: Weekly ES&H Toolbox TalkrjlafortezaNessuna valutazione finora
- Vertical Longlining FishingDocumento72 pagineVertical Longlining FishingEny Duta100% (1)