Potrebbero piacerti anche
- OB Drugs 2263Documento43 pagineOB Drugs 2263Anthony Torres100% (5)
- Spay Neuter PaperDocumento7 pagineSpay Neuter Paperapi-260359232Nessuna valutazione finora
- IV Push MedicationsDocumento67 pagineIV Push Medicationsbtalera100% (1)
- What Is Healing?Documento33 pagineWhat Is Healing?Chef Jem100% (1)
- Prescribing Antibiotics and Analgesics in ChildrenDocumento4 paginePrescribing Antibiotics and Analgesics in ChildrenPreetam PatnalaNessuna valutazione finora
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryDa EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNessuna valutazione finora
- 1st Week ReflectionDocumento2 pagine1st Week Reflectionacharyaamrit0780% (5)
- w15 - Drug StudyDocumento4 paginew15 - Drug StudyGeneva LatorreNessuna valutazione finora
- Appendix 10 Patient Profile TemplateDocumento6 pagineAppendix 10 Patient Profile TemplateAL Rizwan AsifNessuna valutazione finora
- Clubfoot - Ponseti Management. Editor Lynn Stahelli (2003)Documento32 pagineClubfoot - Ponseti Management. Editor Lynn Stahelli (2003)amalia_utami_1Nessuna valutazione finora
- Educational Strategies For Children With Emotional and Behavioral ProblemsDocumento74 pagineEducational Strategies For Children With Emotional and Behavioral Problemsmaeydel50% (2)
- Rheumatologic Disorders: OsteoporosisDocumento7 pagineRheumatologic Disorders: Osteoporosisمحمد رحمان محمد الدليميNessuna valutazione finora
- SR 2Documento33 pagineSR 2hussein alnasryNessuna valutazione finora
- 3 OsteoporosisDocumento6 pagine3 Osteoporosisiraqeana100100Nessuna valutazione finora
- Generic Name: Classification: Prototype of Drug: Brands Available: DosageDocumento3 pagineGeneric Name: Classification: Prototype of Drug: Brands Available: DosageAaliyah OralloNessuna valutazione finora
- Osteoporosis Clinical Case by SlidesgoDocumento30 pagineOsteoporosis Clinical Case by SlidesgoHussein Al-jmrawiNessuna valutazione finora
- Paediatric Pam I DR On Ate IV MonographDocumento2 paginePaediatric Pam I DR On Ate IV MonographDouglas MutenyoNessuna valutazione finora
- Gout and HyperuricemiaDocumento7 pagineGout and HyperuricemiaTaj lamajedNessuna valutazione finora
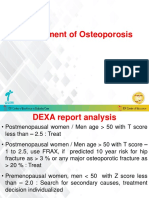
- Management of OsteoporosisDocumento35 pagineManagement of OsteoporosisAKSHAT GARGNessuna valutazione finora
- Alendronate SodiumDocumento3 pagineAlendronate SodiumGLen Caniedo100% (1)
- Masculoskeletal Disorders PharmacotherapyDocumento101 pagineMasculoskeletal Disorders PharmacotherapyWaaqoo Guutuu Waaqoo GuutuuNessuna valutazione finora
- Osteoporosis Treatment and Prevention OptionsDocumento55 pagineOsteoporosis Treatment and Prevention OptionsFarhan FauziNessuna valutazione finora
- OsteoporosisDocumento24 pagineOsteoporosisMousa SuhailNessuna valutazione finora
- Vitamin D TherapyDocumento7 pagineVitamin D Therapydoos1Nessuna valutazione finora
- Drug StudyDocumento8 pagineDrug Studymaryhiromi10Nessuna valutazione finora
- Osteitis DeformansDocumento4 pagineOsteitis Deformansmhuggnetoh19Nessuna valutazione finora
- Vitamin C (Ascorbic Acid) : Drug Information: Pharmacologic Category Dosing: AdultDocumento6 pagineVitamin C (Ascorbic Acid) : Drug Information: Pharmacologic Category Dosing: AdultVictoria Eliza InguilloNessuna valutazione finora
- BisphosphonateDocumento33 pagineBisphosphonatelavate amol bhimraoNessuna valutazione finora
- Metabolic Bone Disorders: By: DR - Shaheen Ahmed Dept of Oral SurgeryDocumento33 pagineMetabolic Bone Disorders: By: DR - Shaheen Ahmed Dept of Oral SurgeryhumaNessuna valutazione finora
- Bone DiseaseDocumento33 pagineBone DiseaseNoor-E-Khadiza ShamaNessuna valutazione finora
- Handbook of Clinical Drug Data 10th Edition Dosage GuideDocumento21 pagineHandbook of Clinical Drug Data 10th Edition Dosage GuideYulia Putri CarlianaNessuna valutazione finora
- Calcium GluconateDocumento9 pagineCalcium Gluconatemarkus_danusantosoNessuna valutazione finora
- OsteoporosisDocumento15 pagineOsteoporosisWil LesterNessuna valutazione finora
- Mineral Homeostasis and Bone TurnoverDocumento43 pagineMineral Homeostasis and Bone TurnoverDylan MansillaNessuna valutazione finora
- Zinc Sulfate: Drug Information: Pharmacologic CategoryDocumento5 pagineZinc Sulfate: Drug Information: Pharmacologic CategoryVictoria Eliza InguilloNessuna valutazione finora
- DenosumabDocumento11 pagineDenosumabVivek ChNessuna valutazione finora
- Colistimethate Sodium 1 Million I.U. Powder For Solution For Injection - Colistin - (Emc)Documento8 pagineColistimethate Sodium 1 Million I.U. Powder For Solution For Injection - Colistin - (Emc)hakim shaikhNessuna valutazione finora
- Steroids in DentistryDocumento4 pagineSteroids in DentistryrazasiddiqueNessuna valutazione finora
- HypophosphataemiaDocumento4 pagineHypophosphataemiaLütfiye ÖzlemNessuna valutazione finora
- OP ملونة كاملةDocumento27 pagineOP ملونة كاملةArcangela QuaintrelleNessuna valutazione finora
- CKD My PharmacotherapyDocumento7 pagineCKD My PharmacotherapyJA TongNessuna valutazione finora
- Presentation On Osteoporosis: Submitted To: Dr. Divya Vohra Submitted By: Sharique Raza M.pharm Jamia HamdardDocumento38 paginePresentation On Osteoporosis: Submitted To: Dr. Divya Vohra Submitted By: Sharique Raza M.pharm Jamia Hamdardsri susantiiNessuna valutazione finora
- Class Indications:: VoriconazoleDocumento3 pagineClass Indications:: VoriconazoleRidha ZharfanNessuna valutazione finora
- OsteoporosisDocumento22 pagineOsteoporosisPrachi DSaNessuna valutazione finora
- Class Indications: MetronidazoleDocumento3 pagineClass Indications: MetronidazoleDwi WulandariNessuna valutazione finora
- Zoledronic Acid InfoDocumento3 pagineZoledronic Acid InfoPratik R JobaliaNessuna valutazione finora
- Drug Literature On OsteoporosisDocumento4 pagineDrug Literature On OsteoporosisRinta MoonNessuna valutazione finora
- Merck Manual: Professional VersionDocumento9 pagineMerck Manual: Professional VersionDwina Wiranti PutriNessuna valutazione finora
- Phenytoin dosage guide for seizures, arrhythmias & moreDocumento4 paginePhenytoin dosage guide for seizures, arrhythmias & moreHarish Ayu LNessuna valutazione finora
- Metoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDocumento9 pagineMetoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDominique RamosNessuna valutazione finora
- Metoclopramide uses and dosageDocumento9 pagineMetoclopramide uses and dosageDominique RamosNessuna valutazione finora
- Health Conditions Health Conditions Alzheimer's & Dementia Anxiety Arthritis Asthma & Allergies Breast Cancer Cancer Cardiovascular Health COVID-19Documento52 pagineHealth Conditions Health Conditions Alzheimer's & Dementia Anxiety Arthritis Asthma & Allergies Breast Cancer Cancer Cardiovascular Health COVID-19BSRT1A BERBANO, IAN JEWEL M.Nessuna valutazione finora
- L 51 R Hypercvad R MaDocumento7 pagineL 51 R Hypercvad R MaMohamed MahmoudNessuna valutazione finora
- Alendronate Study on Bone LossDocumento12 pagineAlendronate Study on Bone LossTrio San LuisNessuna valutazione finora
- Procedure For The Infusion of Biphosphonate Drugs in Clinical Oncology OutpatientsDocumento12 pagineProcedure For The Infusion of Biphosphonate Drugs in Clinical Oncology OutpatientsJyothsna S ReddyNessuna valutazione finora
- Aclasta Drug PresentationDocumento23 pagineAclasta Drug Presentationphp_czarina04421Nessuna valutazione finora
- Tranexamic AcidDocumento3 pagineTranexamic AcidSebastian CruzNessuna valutazione finora
- Exercise Book in Pharmacotherapy 1Documento29 pagineExercise Book in Pharmacotherapy 1Ibtissame BadadNessuna valutazione finora
- Assignment in Pharma Agasbsn2-ADocumento4 pagineAssignment in Pharma Agasbsn2-AMahdiyah AgasNessuna valutazione finora
- Vitamin D Dosing Guide for Deficiency TreatmentDocumento4 pagineVitamin D Dosing Guide for Deficiency TreatmentwiamNessuna valutazione finora
- CDC CiprofloxacinDocumento5 pagineCDC CiprofloxacinIwi DancelNessuna valutazione finora
- Magnesium SulfateDocumento2 pagineMagnesium SulfateKarla Karina Dela CruzNessuna valutazione finora
- Drugs For Bone MetabolismDocumento15 pagineDrugs For Bone MetabolismkwennybiangNessuna valutazione finora
- Vitamin D DeficiencyDocumento4 pagineVitamin D DeficiencyBaba AhmadNessuna valutazione finora
- Intig-D Tablets-SuspensionDocumento2 pagineIntig-D Tablets-Suspensionsweetsmarts85Nessuna valutazione finora
- Fosamax Plus FinalDocumento5 pagineFosamax Plus FinalRobin LimNessuna valutazione finora
- Revised Interpretation of ResultsDocumento27 pagineRevised Interpretation of ResultsSunil Kumar PdNessuna valutazione finora
- PCLRDocumento12 paginePCLRSunil Kumar PdNessuna valutazione finora
- Ankle TraumaDocumento2 pagineAnkle TraumaSunil Kumar PdNessuna valutazione finora
- Bone and Joint TBDocumento15 pagineBone and Joint TBSunil Kumar PdNessuna valutazione finora
- Recurrent Dislocation PatellaDocumento16 pagineRecurrent Dislocation PatellaSunil Kumar PdNessuna valutazione finora
- Claw HandDocumento25 pagineClaw HandSunil Kumar PdNessuna valutazione finora
- Acl Injury and It's ManagementDocumento129 pagineAcl Injury and It's ManagementSunil Kumar PdNessuna valutazione finora
- Republika NG PilipinasDocumento2 pagineRepublika NG PilipinasAcii monseNessuna valutazione finora
- Approaches To The Diagnosis of Portal HipertensionDocumento12 pagineApproaches To The Diagnosis of Portal HipertensionValentina IorgaNessuna valutazione finora
- CDI For ARIADocumento3 pagineCDI For ARIAAshish SharmaNessuna valutazione finora
- Pharmacology: A Career inDocumento2 paginePharmacology: A Career insnikt7863443Nessuna valutazione finora
- Cook 2009 Oropharyngeal DysphagiaDocumento21 pagineCook 2009 Oropharyngeal DysphagiaDesiré MagalhãesNessuna valutazione finora
- ALLIANCE DEFENSE FUND Demand Letter REGARDING CARYN DUTTON, M.D. AND PLANNED PARENTHOOD IN WISCONSINDocumento6 pagineALLIANCE DEFENSE FUND Demand Letter REGARDING CARYN DUTTON, M.D. AND PLANNED PARENTHOOD IN WISCONSINcrush2482Nessuna valutazione finora
- Liver Abscess ThesisDocumento7 pagineLiver Abscess Thesisjenniferalexanderfortlauderdale100% (1)
- Normalised Schemas and Revised ER Diagram for Hospital Management SystemDocumento8 pagineNormalised Schemas and Revised ER Diagram for Hospital Management SystemHenok BayuNessuna valutazione finora
- 4 Coercion in Mental Healthcare The Principle of Least Coercive CareDocumento8 pagine4 Coercion in Mental Healthcare The Principle of Least Coercive CarePedro Y. LuyoNessuna valutazione finora
- SCARED Form ScoringDocumento1 paginaSCARED Form ScoringKaty PuiuNessuna valutazione finora
- Specifications For Civic Education in Primary School PDFDocumento44 pagineSpecifications For Civic Education in Primary School PDFNordiana Abd RahmanNessuna valutazione finora
- STROKE AND TRANSIENT ISCHEMIC ATTACK-dikonversi-dikonversiDocumento5 pagineSTROKE AND TRANSIENT ISCHEMIC ATTACK-dikonversi-dikonversiOcing TanNessuna valutazione finora
- MAPEH 1 (2nd Quarter Complete)Documento60 pagineMAPEH 1 (2nd Quarter Complete)Roselyn GutasNessuna valutazione finora
- 5ОМ англ ВОП 1Documento22 pagine5ОМ англ ВОП 1p69b24hy8pNessuna valutazione finora
- Lab Activity #8Documento3 pagineLab Activity #8Kristelito Grace MarinoNessuna valutazione finora
- Daftar AntibiotikDocumento448 pagineDaftar AntibiotikevaNessuna valutazione finora
- Teacher's Guide: To The Magnificent Mei and Friends Comic SeriesDocumento44 pagineTeacher's Guide: To The Magnificent Mei and Friends Comic SeriesVarizka SalsabilaNessuna valutazione finora
- CV - Chandra Mohan GuptaDocumento4 pagineCV - Chandra Mohan GuptavarunNessuna valutazione finora
- Acetylsalicilic Acid 500mg (Aspirin 500)Documento8 pagineAcetylsalicilic Acid 500mg (Aspirin 500)asdwasdNessuna valutazione finora
- Disaster Readiness and Risk Reduction: Quarter 1-Module 3: Disasters and Its EffectsDocumento11 pagineDisaster Readiness and Risk Reduction: Quarter 1-Module 3: Disasters and Its EffectsRenzelle Guilaran GerocheNessuna valutazione finora
- Maternal and Child Health CareDocumento12 pagineMaternal and Child Health CarePraachii SharmaNessuna valutazione finora
- Mammograms and Other Breast Imaging Procedures: What Is A Mammogram?Documento25 pagineMammograms and Other Breast Imaging Procedures: What Is A Mammogram?Marina StosicNessuna valutazione finora
- Ovr New MohDocumento2 pagineOvr New MohhyNessuna valutazione finora
- Mental Health ResourcesDocumento5 pagineMental Health ResourcesAnna R ZahorNessuna valutazione finora
- Acacia Tree Bark Effective Teeth Whitening AgentDocumento1 paginaAcacia Tree Bark Effective Teeth Whitening Agentarnel100% (1)