Potrebbero piacerti anche
- New Horizons PDFDocumento28 pagineNew Horizons PDFKavooNessuna valutazione finora
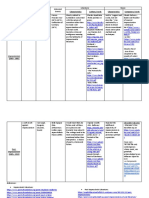
- Period or Movement Characteristics Chief Artists and Major Works Historical Events Literature MusicDocumento2 paginePeriod or Movement Characteristics Chief Artists and Major Works Historical Events Literature Musicsmiley100% (1)
- Translational Systems Biology: Concepts and Practice for the Future of Biomedical ResearchDa EverandTranslational Systems Biology: Concepts and Practice for the Future of Biomedical ResearchNessuna valutazione finora
- Coma and Near-Death Experience: The Beautiful, Disturbing, and Dangerous World of the UnconsciousDa EverandComa and Near-Death Experience: The Beautiful, Disturbing, and Dangerous World of the UnconsciousNessuna valutazione finora
- Elivate Your Life: 7 Keys to Spiritual and Personal TransformationDa EverandElivate Your Life: 7 Keys to Spiritual and Personal TransformationNessuna valutazione finora
- Wit and Humor of the Bible A Literary StudyDa EverandWit and Humor of the Bible A Literary StudyNessuna valutazione finora
- Sink or Swing: Working Out When Life Isn't Working Out: Home Gym Strong, #2Da EverandSink or Swing: Working Out When Life Isn't Working Out: Home Gym Strong, #2Nessuna valutazione finora
- ImpressionismDocumento1 paginaImpressionismSamirAldanaNessuna valutazione finora
- Sonatina y Variacion by - Torroba Fredrico Moreno - Fingered-Andres SegoviaDocumento10 pagineSonatina y Variacion by - Torroba Fredrico Moreno - Fingered-Andres SegoviaKeith Rhodes0% (1)
- G Oster - Auditory Beats in The BrainDocumento19 pagineG Oster - Auditory Beats in The BrainCeci_SunshineNessuna valutazione finora
- T'hooft Quantum Mechanics and DeterminismDocumento13 pagineT'hooft Quantum Mechanics and Determinismaud_philNessuna valutazione finora
- Will Brink - Creatine ReportDocumento43 pagineWill Brink - Creatine ReportDusmanescu Nicolae100% (1)
- Notes To Good Calories Bad CaloriesDocumento30 pagineNotes To Good Calories Bad CaloriesIoana BorceaNessuna valutazione finora
- BRIZO - For Prostate Health PDFDocumento35 pagineBRIZO - For Prostate Health PDFLaychoNessuna valutazione finora
- ةيلكلا: ىعيبطلا جلاعلا ةقرفلا: ةيناثلا ةبعشلا: ةماعلا ررقملا: Exercise physiologyDocumento10 pagineةيلكلا: ىعيبطلا جلاعلا ةقرفلا: ةيناثلا ةبعشلا: ةماعلا ررقملا: Exercise physiologyAhmed abdinNessuna valutazione finora
- Skrabanek Death of Humane MedicineDocumento215 pagineSkrabanek Death of Humane Medicineborg5Nessuna valutazione finora
- Essentials of HeuristicsDocumento233 pagineEssentials of HeuristicsAbidin Zein100% (1)
- Guide For Good Prostate HealthDocumento9 pagineGuide For Good Prostate HealthAlceir FerreiraNessuna valutazione finora
- Cynicism & Winning Isn't NormalDocumento1 paginaCynicism & Winning Isn't NormalPetre BarleaNessuna valutazione finora
- The Food and Supp Coronavirus Version 5.0Documento59 pagineThe Food and Supp Coronavirus Version 5.0Ed RibeiroNessuna valutazione finora
- Galaxy Morphology: By: Amie Sulaiman Saron Ephraim Stephannie GrijalvaDocumento16 pagineGalaxy Morphology: By: Amie Sulaiman Saron Ephraim Stephannie GrijalvaBudi AfriyansyahNessuna valutazione finora
- 00 Cosmology - Cambridge Lecture Notes PDFDocumento82 pagine00 Cosmology - Cambridge Lecture Notes PDFJAY SINGHAM100% (1)
- Homemade Liposomal CDocumento8 pagineHomemade Liposomal CDennis LipterNessuna valutazione finora
- On Physics, Physicists and Philosophy PDFDocumento296 pagineOn Physics, Physicists and Philosophy PDFbabasutarNessuna valutazione finora
- Blend CJC-1295 Ipamorelin The Breakdown of Each PeptideDocumento2 pagineBlend CJC-1295 Ipamorelin The Breakdown of Each Peptidehaydunn55Nessuna valutazione finora
- HOW INVENTION BEGINS ECHOES OF OLD VOICES IN THE RISE OF NEW MACHINES - John H LienhardDocumento288 pagineHOW INVENTION BEGINS ECHOES OF OLD VOICES IN THE RISE OF NEW MACHINES - John H LienhardClara OrtizNessuna valutazione finora
- The Eighteen Arbitrary Parameters of The Standard Model in Your Everyday LifeDocumento9 pagineThe Eighteen Arbitrary Parameters of The Standard Model in Your Everyday LifeM Jesús RodelgoNessuna valutazione finora
- FallonMorell SeminarFinalPartIDocumento183 pagineFallonMorell SeminarFinalPartIMikhail Podduev100% (1)
- Big Bang Theory jhuytttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttffffffffffffffffffffffffffffffxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxbbbbbbbbbbbbbbbbbbbbbdssssssssssssssssssssdmjkgfffffffffffffffffDocumento32 pagineBig Bang Theory jhuytttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttffffffffffffffffffffffffffffffxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxbbbbbbbbbbbbbbbbbbbbbdssssssssssssssssssssdmjkgfffffffffffffffffSwaraj PandaNessuna valutazione finora
- Uffe Ravnskov Ignore The AwkwardDocumento98 pagineUffe Ravnskov Ignore The Awkwardjha.sofcon5941100% (3)
- Mass in A Flash 2.0 PDFDocumento16 pagineMass in A Flash 2.0 PDFArjun SinghNessuna valutazione finora
- Triple Positive Breast Cancer - ViciDocumento8 pagineTriple Positive Breast Cancer - ViciEmilio AlaquàsNessuna valutazione finora
- The Diverse Consequences of Aneuploidy PDFDocumento9 pagineThe Diverse Consequences of Aneuploidy PDFAndriel CardosoNessuna valutazione finora
- Definition:: - Lipids Are Organic Compounds FormedDocumento13 pagineDefinition:: - Lipids Are Organic Compounds FormedSimmiNessuna valutazione finora
- MiHealth TechnologyDocumento11 pagineMiHealth Technologymartinpacenza32Nessuna valutazione finora
- Li Hong Zie BiografiDocumento11 pagineLi Hong Zie BiografiJiwen SalimNessuna valutazione finora
- Gut The Inside Story of Our Body S Most Underrated OrganDocumento5 pagineGut The Inside Story of Our Body S Most Underrated Organjeph79100% (1)
- Sonus Diabetes Secret Review Karen Richardson Real OrywcocbxxgxDocumento2 pagineSonus Diabetes Secret Review Karen Richardson Real Orywcocbxxgxlutesail7Nessuna valutazione finora
- DopamineDocumento128 pagineDopamineJordan Moshcovitis100% (3)
- The Ultimate Guide To Biohacking Exercise With Oxygen Therapy, Hypoxia, Elevation & Altitude TrainingDocumento17 pagineThe Ultimate Guide To Biohacking Exercise With Oxygen Therapy, Hypoxia, Elevation & Altitude TrainingAlessandro QuercettiNessuna valutazione finora
- Steroids JenniferKettelDocumento25 pagineSteroids JenniferKettelvinay0717Nessuna valutazione finora
- White Paper-Child ObesityDocumento14 pagineWhite Paper-Child Obesityapi-252262472Nessuna valutazione finora
- Irwin Stone: Food Preservative WorkDocumento3 pagineIrwin Stone: Food Preservative WorkxfucvuehNessuna valutazione finora
- Line 6 - HX Stomp Manual - EnglishDocumento52 pagineLine 6 - HX Stomp Manual - EnglishLorena DiazNessuna valutazione finora
- Lloyd Bud Winter: Sleep Deprivation StatisticsDocumento1 paginaLloyd Bud Winter: Sleep Deprivation Statisticsanna100% (1)
- Checklist - Hyperbaric Treatment For Children With Autism A MulticenterDocumento3 pagineChecklist - Hyperbaric Treatment For Children With Autism A MulticenterJim GoetzNessuna valutazione finora
- Nutrition and Disease: A Mediterranean Diet Is Cost-Effective in Patients With Previous Myocardial InfarctionDocumento7 pagineNutrition and Disease: A Mediterranean Diet Is Cost-Effective in Patients With Previous Myocardial InfarctionRenato CastillaNessuna valutazione finora
- Primary Prevention of Cardiovascular Disease With A Mediterranean DietDocumento7 paginePrimary Prevention of Cardiovascular Disease With A Mediterranean DietKartika HeruNessuna valutazione finora
- Long-Term Follow-Up After Tight Control of Blood Pressure in Type 2 DiabetesDocumento12 pagineLong-Term Follow-Up After Tight Control of Blood Pressure in Type 2 DiabetesnovywardanaNessuna valutazione finora
- CometDocumento9 pagineCometSohail AhmedNessuna valutazione finora
- Nejmoa 021778Documento11 pagineNejmoa 021778aandakuNessuna valutazione finora
- New England Journal Medicine: The ofDocumento11 pagineNew England Journal Medicine: The ofGonzalo LealNessuna valutazione finora
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyDa EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyValutazione: 1 su 5 stelle1/5 (1)
- Effects of Diet and Simvastatin On Serum Lipids, Insulin, and Antioxidants in Hypercholesterolemic MenDocumento8 pagineEffects of Diet and Simvastatin On Serum Lipids, Insulin, and Antioxidants in Hypercholesterolemic MenAranel BomNessuna valutazione finora
- Michael E. Mann Curriculum Vitae With Funding / Grant InformationDocumento26 pagineMichael E. Mann Curriculum Vitae With Funding / Grant InformationacolpoNessuna valutazione finora
- Heywood 2012 PDFDocumento6 pagineHeywood 2012 PDFacolpoNessuna valutazione finora
- B12 - Hallelujah - Donaldson 2000 PDFDocumento6 pagineB12 - Hallelujah - Donaldson 2000 PDFacolpoNessuna valutazione finora
- How Prevalent Is Vitamin B 12 Deficiency Among Vegetarians? - Pawlak 2013Documento8 pagineHow Prevalent Is Vitamin B 12 Deficiency Among Vegetarians? - Pawlak 2013acolpoNessuna valutazione finora
- Vegan Diet, Subnormal Vitamin B-12 Status and Cardiovascular Health - Woo 2012Documento15 pagineVegan Diet, Subnormal Vitamin B-12 Status and Cardiovascular Health - Woo 2012acolpoNessuna valutazione finora
- ACCIDENTS ON MAIN RURAL HIGHWAYS RELATED TO SPEED, DRIVER, and VEHICLE - David Solomon, 1964Documento50 pagineACCIDENTS ON MAIN RURAL HIGHWAYS RELATED TO SPEED, DRIVER, and VEHICLE - David Solomon, 1964acolpoNessuna valutazione finora
- ITE Speed Zoning GuidelinesDocumento4 pagineITE Speed Zoning GuidelinesacolpoNessuna valutazione finora
- Hydrogenation PDFDocumento18 pagineHydrogenation PDFAle SanzNessuna valutazione finora
- Basic Concepts of NutritionDocumento23 pagineBasic Concepts of NutritionMarie Nelle Escriba Limpoco50% (2)
- Proceedings 10th Mountain Cheese DefDocumento95 pagineProceedings 10th Mountain Cheese DefLazline BrownNessuna valutazione finora
- FatsDocumento6 pagineFatsro_sheenNessuna valutazione finora
- Teds Bunge Amaizing Ss Bu-504Documento2 pagineTeds Bunge Amaizing Ss Bu-504api-226773621Nessuna valutazione finora
- Table of Alimentary OilsDocumento3 pagineTable of Alimentary Oilshonest_loezNessuna valutazione finora
- Chemistry of Oils & Fats and Their Health Effects: Rummi Devi SainiDocumento16 pagineChemistry of Oils & Fats and Their Health Effects: Rummi Devi SainiKasirao MScNessuna valutazione finora
- Specimen Bmat 2016 Past Paper Section 1 PDFDocumento28 pagineSpecimen Bmat 2016 Past Paper Section 1 PDFSkruzdelyte MielaNessuna valutazione finora
- The Oiling of AmericaDocumento26 pagineThe Oiling of Americalinandstacey100% (1)
- Che 402: Analytical ChemistryDocumento12 pagineChe 402: Analytical ChemistryKrizzete HernandezNessuna valutazione finora
- Set 2Documento10 pagineSet 2babu singhNessuna valutazione finora
- Fats and Fatty Acids in Poultry Nutrition and Health - 2Documento21 pagineFats and Fatty Acids in Poultry Nutrition and Health - 2MuhammadFarrukhHafeez0% (1)
- Cooking Oil MeasurementDocumento33 pagineCooking Oil Measurementblack_knight728100% (3)
- Biodiesel Density PDFDocumento8 pagineBiodiesel Density PDFFernandoNessuna valutazione finora
- Greenlandic Inuit Show Genetic Signatures of Diet and Climate AdaptationDocumento1 paginaGreenlandic Inuit Show Genetic Signatures of Diet and Climate AdaptationCates MandinNessuna valutazione finora
- 7 - Structur Lipid & As. Lemak TrisuspptDocumento47 pagine7 - Structur Lipid & As. Lemak TrisuspptNurul Sukmaning HabibieNessuna valutazione finora
- Food Facts and FallaciesDocumento12 pagineFood Facts and FallaciesAbigail AnziaNessuna valutazione finora
- 180 Muscle Weight Gain MethodDocumento19 pagine180 Muscle Weight Gain MethodCecilio GutierrezNessuna valutazione finora
- Fat Facts PDFDocumento6 pagineFat Facts PDFEko Ariyanto Wong PlembangNessuna valutazione finora
- Rice Bran Oil - Natures Gift To MankindDocumento2 pagineRice Bran Oil - Natures Gift To Mankindlehmanwolf100% (1)
- Fatty Acid CompositionDocumento5 pagineFatty Acid CompositionAnonymous MhTaJsNessuna valutazione finora
- Our Objective: What Are Fatty Acids?Documento5 pagineOur Objective: What Are Fatty Acids?Sunita MauryaNessuna valutazione finora
- The Bear PDFDocumento318 pagineThe Bear PDFjoeNessuna valutazione finora
- Pink Panther - Diabetes Management - Chapter 11Documento18 paginePink Panther - Diabetes Management - Chapter 11jennmoyerNessuna valutazione finora
- Nuts and Seeds in Health and Disease Prevention - Chapter 4Documento11 pagineNuts and Seeds in Health and Disease Prevention - Chapter 4Wendy YangNessuna valutazione finora
- C.H.A. Diet - Vol.2Documento62 pagineC.H.A. Diet - Vol.2Sixp8ck100% (3)
- Research Paper On Cooking OilDocumento8 pagineResearch Paper On Cooking Oilgw21tcyd100% (1)
- The Junk Science Self Defense Manual by Anthony ColpoDocumento30 pagineThe Junk Science Self Defense Manual by Anthony ColpoacolpoNessuna valutazione finora
- Cholesterol MythDocumento31 pagineCholesterol Mythajaysuperking100% (4)
- Chemistry Higher Level Chapter 17Documento52 pagineChemistry Higher Level Chapter 17Caryl Alvarado SilangNessuna valutazione finora